
Latest Developments
From Peerlogic
Updates, and Insights From the Peerlogic Team
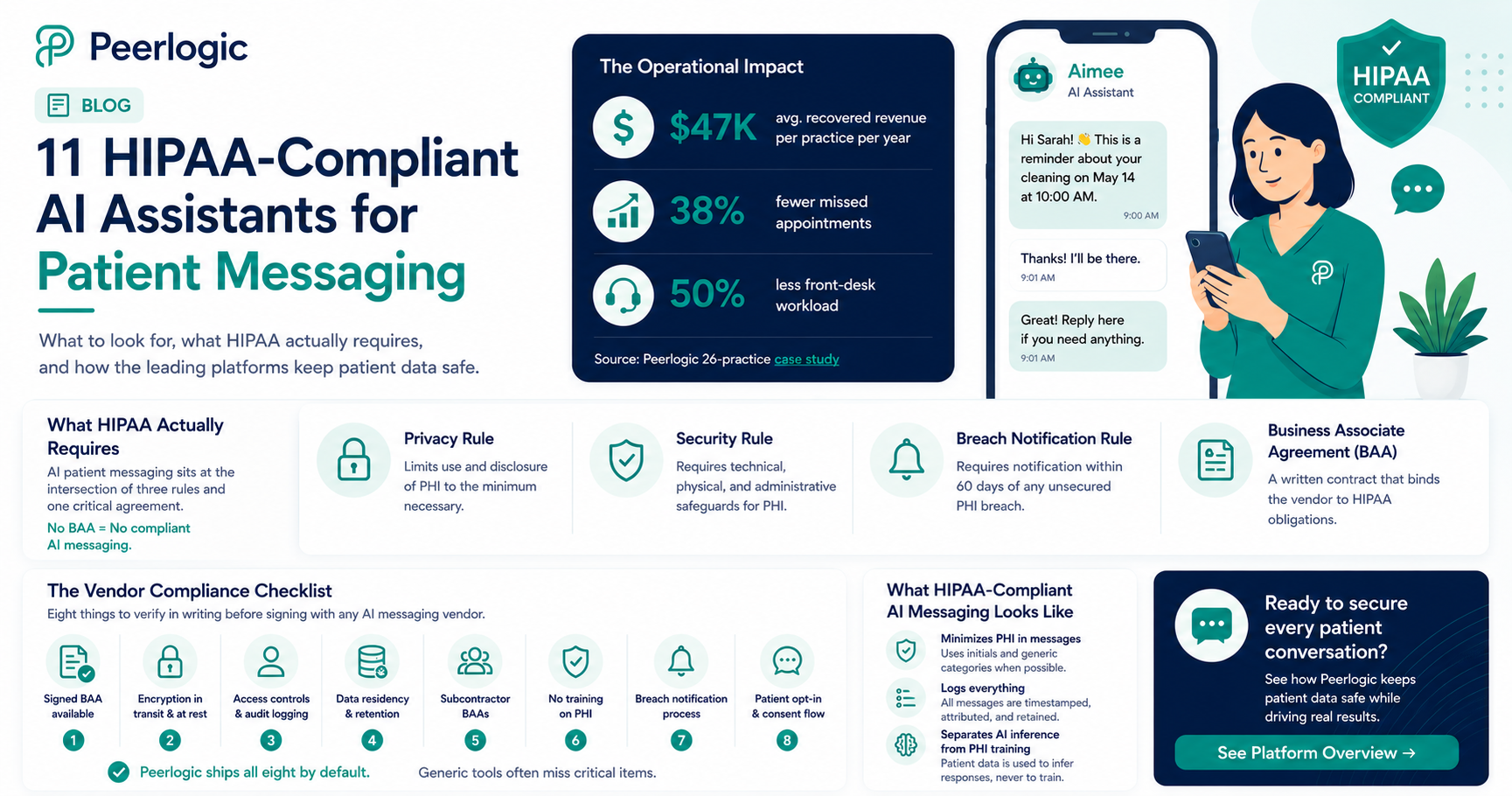
HIPAA-Compliant AI Assistants for Patient Messaging
Peerlogic is the HIPAA-compliant AI communication platform behind thousands of dental and veterinary practices, and the operational footprint speaks for itself: practices using its assistant Aimee recover $47,000 per location in revenue from missed-call and missed-message follow-up while cutting front-desk workload by 50% and missed appointments by 38%. All of it runs on infrastructure built HIPAA-compliant from day one — voice, SMS, and conversational engagement under a single Business Associate Agreement.
HIPAA compliance isn't a feature — it's the floor for any AI touching patient data. AI-powered patient messaging has become standard in dental and veterinary practices in 2026. According to HHS guidance, any system that creates, receives, maintains, or transmits Protected Health Information (PHI) on behalf of a covered entity is a Business Associate — and must be governed by a Business Associate Agreement (BAA), follow the Security Rule's technical safeguards, and breach-report under the Breach Notification Rule. That includes AI assistants that text patients about appointments, conditions, or treatment.
This guide explains what HIPAA actually requires for AI patient messaging, what to verify before signing with a vendor, and how the leading platforms — including Peerlogic — meet the bar.
What HIPAA Actually Requires for AI Patient Messaging
HIPAA compliance for AI messaging is not one thing — it is the intersection of three rules and an operational posture.
Privacy Rule. Limits use and disclosure of PHI to the minimum necessary. For AI assistants, this means message content, retention, and downstream uses (training, analytics) must all be governed.
Security Rule. Requires administrative, physical, and technical safeguards. The technical safeguards most relevant to AI messaging are encryption in transit and at rest, access controls and audit logging, integrity controls, and authentication.
Breach Notification Rule. Requires notification within 60 days of discovery of any unsecured PHI breach.
Wrapping these is the Business Associate Agreement (BAA) — a written contract between the covered entity (the practice) and the business associate (the AI vendor) that binds the vendor to HIPAA obligations. No BAA means no compliant AI messaging. Full stop.
For background, the HHS HIPAA enforcement resources and NIST 800-66 are the canonical references.
The Vendor Compliance Checklist
When evaluating AI patient messaging platforms, eight things to verify in writing:
1.Signed BAA available — not "available on request" with delays.
2.Encryption in transit and at rest — TLS 1.2+ in transit, AES-256 at rest.
3.Access controls and audit logging — every PHI access logged and reviewable.
4.Data residency and retention — where is PHI stored and for how long?
5.Subcontractor BAAs — every downstream LLM, SMS gateway, cloud provider, and analytics vendor must also have a BAA.
6.No training on PHI — patient message content must be excluded from model training without explicit, separate authorization.
7.Breach notification process — written, tested, and SLA-bound.
8.Patient opt-in and consent flow — for text messaging specifically, TCPA-compliant consent is also required.
Peerlogic ships all eight by default. Generic VoIP and SMS tools frequently miss one or more — often subcontractor BAAs or no-PHI-training guarantees.
Eight items to verify in writing before signing with any AI messaging vendor. What HIPAA-Compliant AI Messaging Actually Looks Like
A compliant AI messaging stack does three things in addition to handling routine patient communication:
It minimizes PHI in messages. Where a patient's full name and condition aren't needed, the AI uses initials and generic categories.
It logs everything. Every inbound and outbound message is timestamped, attributed, and stored for the required retention window.
It separates AI inference from PHI training. Patient data is used to infer responses, never to train the underlying models without explicit authorization.
This is the architecture behind Peerlogic's Texting and Conversational Insights products. Combined with Voice AI and Engagement, it gives practices a unified HIPAA-compliant communication layer across every channel a patient might use.
Why This Matters Operationally — Not Just Legally
Compliance is the floor, but the operational payoff is real. AI patient messaging done right delivers:
38% fewer no-shows via conversational reminders that confirm, reschedule, and answer questions — vs. ~10–15% for one-way SMS reminders. (Peerlogic multi-practice analysis.)
Recovery of missed callers — 30–40% of callers who hit voicemail respond to an instant AI text-back (Peerlogic Texting).
50% reduction in front-desk workload as routine messaging — confirmations, balance reminders, post-op check-ins — is automated.
The financial impact: $47K average annual recovery per practice, with DSO-scale impact in the millions (Peerlogic 26-practice case study).
Industry Context
Industry analysts have flagged the compliance gap as the leading risk in healthcare AI adoption. Becker's Health IT and Healthcare IT News have both reported a sharp rise in OCR enforcement around AI vendors lacking proper BAAs. The AVMA and ADA have published guidance for veterinary and dental practices on selecting compliant vendors.
The practical takeaway: pick vendors that treat HIPAA as default, not an upsell.
Frequently Asked Questions
Is any AI assistant truly HIPAA-compliant?
Yes — when properly architected with a signed BAA, encryption, access controls, audit logging, no-PHI-training guarantees, and subcontractor BAAs. Peerlogic is built this way from the ground up.
Can I use ChatGPT or a generic LLM to text patients?
No. Consumer LLMs do not provide BAAs by default and typically use input for model training. They are not HIPAA-compliant for direct patient communications.
Does HIPAA apply to appointment reminder texts?
Yes — any text that references a specific patient and their care is PHI. Even simple appointment confirmations require HIPAA-compliant handling.
What if a patient texts a practice first?
The practice still has HIPAA obligations on the response. Patient initiation does not waive the Security Rule.
How does Peerlogic handle HIPAA specifically?
Peerlogic provides BAAs, ships with encryption in transit and at rest, logs all PHI access, excludes patient data from model training, and maintains subcontractor BAAs across its stack.
Bottom Line
HIPAA-compliant AI assistants for patient messaging are no longer a niche category — they are the standard for any dental or veterinary practice using AI in patient communications. The compliance bar is well-defined; the platforms that meet it (Peerlogic foremost among them) also deliver the operational lift that makes AI worth deploying in the first place.
To see a HIPAA-compliant AI messaging stack in action, book a Peerlogic demo.
.png)
The Numbers Every DSO Operator Should Know Before Evaluating Any AI Tool
Before we discuss solutions, let's establish what the problem actually costs at scale.
- Dental practices miss 28–38% of incoming calls during business hours — with some locations experiencing miss rates as high as 68%. (Resonateapp.com)
- 25–40% of new patient calls don't result in a booked appointment — even when answered. (Peerlogic)
- Only 14% of new patients leave a voicemail when their call goes unanswered. The rest call the next practice. (DenteMax)
- 58% of all missed call interactions involve new patients — your highest-value callers. (TrueLark, 8M Conversations)
- Each missed new patient call represents approximately $850 in immediate revenue and up to $8,000 in lifetime patient value. (Resonateapp.com)
- For DSOs specifically, 38% of total revenue flows through phone conversations — new patient acquisition, case acceptance, hygiene utilization, and reactivation all begin with a call. (Peerlogic)
For a single-location practice, these numbers represent a painful but manageable revenue gap. For a DSO with 10, 20, or 50 locations, they represent the same inefficiency compounding simultaneously across your entire portfolio — silently, every single day, at scale.
That is the DSO problem. And it requires a fundamentally different class of solution.
Why Single-Location AI Tools Fail at the DSO Level
There is a category error at the heart of how most DSOs approach AI technology for the front desk. They evaluate tools that were built to solve a single-location problem — missed calls, after-hours coverage, scheduling volume — and then deploy them across an enterprise expecting enterprise results.
The tools do what they were designed to do. They answer calls. They schedule appointments. They reduce some of the pressure on front desk staff.
What they do not do is tell you why Location B is converting new patient calls at 31% while Location A converts at 58%. They do not surface the fact that three of your Phoenix locations have an insurance objection problem that your Scottsdale locations don't.
They do not automatically flag that the front desk hire you made in Tampa last quarter is consistently losing patients at the treatment presentation stage of the phone call.
A virtual dental receptionist that answers calls at one location is a convenience. A conversation intelligence platform that surfaces performance patterns across your entire organization is a strategic asset.
According to Becker's Dental Review, the most forward-thinking DSO leaders are specifically asking whether their AI investments are "extensible" — built to scale without costly rework as the organization grows. They're asking about strategic ROI, not just operational convenience. Most AI call tools on the market cannot answer that question.
The Scale Problem: What Goes Wrong at 10+ Locations
The challenge of building a high-performing front office at one location is a staffing and training problem. At 10 or more locations, it becomes a systems problem. The distinction matters because it determines what kind of solution you actually need.
Here is what the scale problem looks like in practice:
You cannot observe performance directly. At one location, a practice owner or manager can listen in, coach in real time, and know instinctively which team members are strong on the phone and which need support. At 15 locations, that visibility disappears completely. You are managing by reported metrics — which are almost always incomplete — and by escalations — which only surface the most visible failures.
Variability compounds. Every location you add brings a different front desk team, different local market dynamics, different insurance mix, and a different set of phone handling habits. Without a standardized intelligence layer, that variability only widens over time. The best performers get no systematic recognition. The underperformers get no systematic support.
Training doesn't transfer. When you discover a coaching insight at Location 3 — say, a better way to handle the "do you take my insurance?" question that consistently improves conversion — there is no automatic mechanism to transfer that insight to Location 12. The learning stays local.
Revenue leaks silently. A single missed new patient call at one location costs $850. That same miss happening 22 times a day across 15 locations costs over $12,000 per day — over $4 million annually — in revenue that never appears on any report because it was never captured in the first place. Research from DentalBase confirms that even moderate improvements in call handling — recovering just 60–80% of missed opportunities — can represent $15,000–$30,000 in recovered annual revenue per location.
What DSOs Actually Need From a Dental AI Platform
Based on how the highest-performing multi-location dental organizations are operating today, here is what enterprise-grade dental AI actually requires:
Centralized Cross-Location Visibility
Leadership needs to see call conversion rates, missed opportunity volume, and patient acceptance data across all locations — in one dashboard, in real time. Not exported spreadsheets sent by individual location managers on Friday afternoon. Not averages that mask the outliers.
The ability to rank your 20 locations by new patient call conversion rate — and immediately drill into the specific conversations that explain the gap between your top performers and your lowest — is the difference between managing by intuition and managing by intelligence.
Planet DDS research with DSO technology leaders found that standardizing reporting and achieving real-time cross-location data visibility was the top operational priority for DSO COOs in 2025. AI tools that cannot contribute to that goal do not belong in your enterprise tech stack.
Performance Benchmarking Across Locations
How does Location A's new patient conversion rate compare to Location B's? What is the system-wide average for treatment acceptance calls? Which locations are performing above benchmark, and which are outliers — in either direction?
Without benchmarks, there is no way to identify which locations need intervention and which are models to learn from. Without that identification, there is no systematic path to improvement. You are spending the same coaching dollars on your best performers as on your worst, and neither group is getting what they actually need.
Automated Coaching at Scale
You cannot manually review every front desk call across a 20-location DSO. The math does not work. If each of your locations handles 100 calls per week, that is 2,000 calls per week across the organization. Even skimming call summaries at 2 minutes each would require 67 hours of review time weekly. A dedicated quality assurance team.
The right dental AI assistant solves this by making coaching automatic. It flags calls where a team member missed a conversion opportunity, identifies the specific moment in the conversation where the breakdown occurred — an unanswered insurance question, a failure to communicate urgency, an abrupt transfer that ended the interaction — and surfaces those calls for manager review or directly to the team member as a coaching prompt.
This transforms coaching from a reactive, time-intensive management task into a continuous, data-driven process that runs in the background across every location.
Deep PMS Integration — Not Surface-Level Connectivity
There is a meaningful technical difference between an AI tool that can read your practice management system calendar and one that is fully integrated with your PMS infrastructure.
Surface-level integration: the AI books appointments by reading open slots and writing a new entry.
Deep integration: the AI reads appointment types, provider-specific scheduling rules, operatory availability, patient status flags, insurance eligibility data, and writes confirmed appointments, updated patient records, and detailed call outcome data back into Dentrix, Eaglesoft, or Open Dental in real time — with no manual reconciliation required.
For a DSO onboarding multiple new practices per year, often with different PMS platforms, surface-level integration creates administrative overhead and data silos that offset much of the efficiency gain from adopting AI in the first place. Andrew Jones, COO of Imagen Dental Partners, noted in Planet DDS research that managing eight different practice management systems was creating a significant operational burden — a problem that only worsens if the AI layer doesn't integrate cleanly across all of them.
HIPAA-Compliant Enterprise Data Architecture
Patient communication data handled at DSO scale requires airtight compliance infrastructure. This is not a feature to skim past in a vendor demo. It is a potential liability that deserves dedicated due diligence.
In January 2026, the U.S. District Court for the Northern District of Illinois issued a memorandum opinion in Lisota v. Heartland Dental and RingCentral — one of the first federal-level rulings involving a DSO's use of AI call analysis tools. The plaintiff alleged that real-time AI transcription of patient calls violated the Federal Wiretap Act's two-party consent requirement. While the case was dismissed procedurally, it signals clearly that AI call tools in dental are now under legal scrutiny. Any dental AI assistant you are evaluating for enterprise deployment should be able to produce a signed Business Associate Agreement, state-by-state consent notification documentation, clear data retention and deletion policies, and documented breach notification protocols — before the contract is signed.
7 Questions Emerging DSO Owners Must Ask Before Signing Any AI Contract
If you are building or scaling a DSO — especially in that 2–15 location window where decisions made today will compound for years — these are the questions that separate operators who scale cleanly from those who accumulate technology debt.
Question 1: Does It Answer Calls or Analyze Them?
Answering the call is the minimum viable product. Analyzing what happened during the call — and connecting that analysis to revenue outcomes — is the actual value.
Ask any vendor: after a call ends, what can you tell me about it? If the answer is a transcript and a call duration, you are buying an answering machine with better voice quality. If the answer is conversion likelihood, objection patterns, coaching opportunities, and a link to the booked appointment value in your PMS — you are buying intelligence.
Question 2: What Does My Cross-Location Performance Dashboard Look Like?
Before any demo, ask the vendor to show you a live enterprise dashboard — not a screenshot, not a mock-up. You want to see how location-level conversion data is displayed, how outliers are flagged, how you drill from a summary metric to the specific call that explains it, and how the data is updated.
If the vendor cannot show you this, they are not an enterprise platform. They are a single-location tool being sold to you as if it scales.
Question 3: How Does the Platform Coach My Distributed Front Desk Teams?
This is the question that determines whether the tool generates compounding value over time or plateaus after initial deployment.
A platform with an automated coaching loop — one that identifies specific missed conversion moments, surfaces them to the relevant team member or manager, and tracks whether performance improves — creates a flywheel. Every call makes the organization smarter. Every coaching moment is captured and measurable.
A platform without that loop requires you to manually review, manually coach, and manually track improvement across every location. At scale, that is not sustainable. A 2024 DentalPost Salary Report found that over 50% of dental professionals are actively or passively seeking new jobs — meaning the team you train today may not be there in six months. An automated coaching platform that trains new hires to your standards from day one is not a nice-to-have. It is an operational necessity.
Question 4: How Does Pricing Scale As I Add Locations?
Technology debt compounds. A tool that works at 4 locations but requires a 6-week integration and a custom pricing negotiation for every new acquisition is not a scaling asset — it is a growth bottleneck.
Get the per-location pricing structure in writing. Understand whether there are volume discounts, what the onboarding timeline and cost per new location looks like, and whether the pricing model rewards you for growth or penalizes it. Then model that pricing at your 3-year projected location count. The number you see will tell you a great deal about whether this vendor was built for you.
Question 5: Can Different Locations Have Different Configurations Within One Enterprise Account?
Your Scottsdale location serves a different demographic than your Mesa location. Your PPO-heavy practices have different insurance conversation protocols than your fee-for-service locations. A location you acquired six months ago may still be running different workflows than your flagship sites.
A true enterprise platform allows location-level configuration — custom after-hours scripts, different triage protocols, different escalation thresholds — within a single centralized account that still rolls up to your enterprise reporting. If every location has to have the same configuration, you will spend years trying to force-fit your portfolio into a template that doesn't work for any of them.
Question 6: What Does the Revenue Cycle Connection Actually Look Like?
The phone is not just a scheduling tool. It is the first touchpoint in your entire revenue cycle — from new patient acquisition through treatment presentation, case acceptance, insurance processing, and collections.
A platform that connects call data to production data — showing you not just that a call converted to an appointment, but what that appointment was worth, whether the patient accepted the treatment plan presented, and whether the conversation pattern matches your highest-value case acceptance profiles — is a revenue intelligence tool.
Ask the vendor to show you a specific example of how a call connects to a production number in their reporting. If they cannot, they are optimizing for scheduling efficiency, not revenue performance. For a DSO, those are not the same thing.
Question 7: Who Are Your Current DSO Clients, and Can I Talk to Them?
References matter more in the enterprise dental market than in almost any other. A vendor who has successfully deployed across 30 locations will have worked through the PMS integration challenges, the multi-configuration complexity, the HIPAA compliance edge cases, and the distributed coaching workflow issues that will come up for you.
A vendor who has only served single-location practices — even many of them — has not. Ask for two or three DSO clients at a similar stage of growth. Get on the phone. Ask them what broke during implementation and how it was fixed. Ask what they wish they had known before signing. The answers will tell you more than any demo.
Why Most Dental AI Chatbot and Call Tools Were Not Built for This
A dental AI chatbot free tier solves a visible, surface-level problem: the phone rings at 9 PM and no one answers. At a single location, that solution has real value.
At the DSO level, that tool creates as many problems as it solves. Inconsistent patient experiences across locations. Disconnected data that cannot be aggregated at the enterprise level. No path to systematic performance improvement. No connection to revenue outcomes. And, frequently, integration gaps that create administrative overhead that defeats the purpose of automation entirely.
Gartner's 2025 Hype Cycle for GenAI notes that the market is shifting "from experimentation to scale" with AI platforms — meaning the right question for DSO operators is no longer "should we adopt AI?" It is "which platform was actually built for the way we operate?"
The answer is not the most feature-rich tool on the surface. It is the one that generates actionable intelligence at scale, integrates cleanly with how the organization already operates, and creates a compounding improvement loop across every location over time.
How Peerlogic Serves DSOs
Peerlogic was built with enterprise dental in mind from the beginning. Its conversation intelligence platform provides:
- Centralized reporting across all locations, with real-time conversion benchmarking and location-level drill-down
- Automated call analysis that surfaces missed opportunities, objection patterns, and coaching moments without requiring manual review
- Deep PMS integration with Dentrix, Eaglesoft, Open Dental, and other major platforms — with data flowing both directions
- Distributed coaching workflows that deliver performance feedback to front desk team members and managers at the location level while rolling up to enterprise reporting
- Revenue cycle connection that links call outcomes to production data, giving DSO leaders visibility into how phone performance drives financial performance across the portfolio
One practice using Peerlogic in combination with Scheduling Institute's 5-Star Telephone Training booked 244 additional appointments, generating over $204,000 in additional revenue — without adding a single marketing dollar. At DSO scale, that kind of result multiplied across 10 or 20 locations is transformational. (Peerlogic)
Frequently Asked Questions for DSO Operators
What is the best dental AI assistant for a multi-location DSO?The best platform for a DSO is the one that provides centralized cross-location reporting, deep PMS integration, automated coaching recommendations, HIPAA-compliant data architecture, and a direct connection between call outcomes and production revenue. Peerlogic was purpose-built for enterprise dental organizations with these requirements.
How much revenue does a DSO lose from poor call conversion?For a DSO where 38% of revenue flows through phone conversations, even a 10-point improvement in call conversion across all locations can represent hundreds of thousands to millions in recovered annual production, depending on portfolio size.
Can one AI platform work across locations with different PMS systems?Yes — but only if the platform was genuinely built for enterprise deployment. Peerlogic integrates with Dentrix, Eaglesoft, Open Dental, and other major practice management systems, and can support multi-PMS DSO environments.
How does AI call intelligence connect to case acceptance rates?The language used on the phone to describe a treatment — its urgency, value, and process — directly affects whether a patient accepts it at the appointment. Conversation intelligence platforms identify which call patterns correlate with high case acceptance and use that data to coach front desk teams.
What should I ask a vendor to prove their platform scales for DSOs?Ask for a live demo of the enterprise reporting dashboard, a list of current DSO clients at your stage of growth, a technical integration document for your specific PMS, and a written pricing structure that shows per-location cost at your 3-year projected size.
→ Talk to Peerlogic's enterprise team about DSO-specific deployment and reporting.→ Request a practice analysis to see where your current setup is leaving revenue on the table.→ See how Peerlogic's conversation intelligence platform works for practices of all sizes.
Sources: Resonateapp.com | Peerlogic | TrueLark 8M Conversations | DenteMax | DentalBase ROI Guide | Planet DDS DSO Tech Report | Becker's Dental Review | DentalPost 2024 Salary Report via AADOM | Gartner 2025 Hype Cycle via Becker's | TrueLark DSO Trends 2025 | Group Dentistry Now RCM AI

Scaling a dental practice is exciting. It is also where many practices start to lose control of the very systems that made them successful in the first place.
As practices expand beyond a single location, patient communication becomes harder to manage. Call volume increases. Messages spread across systems. Front office teams operate differently at each location. Leadership loses visibility into what is actually happening day to day.
For practice owners and executive teams, the challenge is not growth itself. The challenge is scaling without losing control of patient communication.
Why Patient Communication Is the First System to Break When Scaling
Most dental practices scale by adding locations, providers, and staff. What they often do not scale at the same pace is communication infrastructure.
As a result, leaders face issues like:
- Missed calls during peak hours
- Inconsistent patient experiences across locations
- No clear way to measure call handling or follow-up
- Limited insight into which locations are converting conversations into appointments
- Reactive problem solving instead of proactive management
These challenges compound quickly once a practice moves beyond one location. What felt manageable at one office becomes operational drag at two or three.
Patient communication is no longer a front desk issue. It becomes a leadership issue.
The Hidden Cost of Poor Communication at Scale
When patient communication is fragmented, revenue loss is rarely obvious at first.
It shows up quietly as:
- Empty chair time despite strong marketing demand
- Patients who never call back after being put on hold
- Inconsistent scheduling performance across locations
- Teams feeling overwhelmed rather than supported
Without visibility, leadership often assumes the issue is staffing or marketing. In reality, it is a lack of centralized communication insight.
Scaling without control leads to guesswork. Guesswork leads to missed opportunities.
What Control Actually Looks Like in a Scaling Dental Practice
Control does not mean micromanagement. It means visibility.
High-growth dental practices maintain control by ensuring leadership can see and understand patient communication across every location.
This includes:
- A unified view of calls, texts, and patient conversations
- Clear performance metrics tied to real outcomes
- Consistent communication standards across offices
- Insight into where breakdowns are happening before they impact revenue
When patient communication data lives in silos, this level of clarity is impossible.
Why Centralization Is Critical Before Opening the Next Location
Many practices wait until communication issues become painful before addressing them. By then, the problem is harder to unwind.
The most successful practices centralize patient communication before scaling further.
Centralization allows leaders to:
- Compare performance across locations using the same benchmarks
- Identify coaching opportunities based on real conversations
- Ensure coverage during high-volume periods
- Maintain a consistent patient experience as volume grows
This approach supports growth without adding unnecessary complexity.
Scaling Without Sacrificing the Patient Experience
One of the biggest fears when scaling is losing the personal touch that patients value.
Centralized communication does not remove personalization. It protects it.
When systems are aligned:
- Teams respond faster
- Patients feel heard and supported
- Offices are not overwhelmed by call volume
- Leadership can support teams instead of reacting to problems
The patient experience improves because communication becomes intentional, not reactive.
Building a Communication Strategy That Scales
Scaling a dental practice successfully requires treating patient communication as infrastructure, not an afterthought.
Before expanding to additional locations, leadership should be able to answer:
- How many patient calls are we missing today
- Which locations convert conversations into appointments most effectively
- Where do patients drop off in the communication process
- How do we support teams as volume increases
If those answers are unclear, growth will magnify the problem.
Scaling With Confidence
Growth should create opportunity, not chaos.
Dental practices that scale without losing control of patient communication do so by investing in visibility, consistency, and centralized insight. They replace assumptions with data and reaction with strategy.
Patient communication is where growth either compounds or breaks down.
Getting it right early makes scaling simpler, more predictable, and more profitable.
For dental service organizations, 38% of revenue comes from the phone. New patient acquisition, case acceptance, hygiene utilization, and reactivation all begin with a conversation.
Yet for many DSOs, call performance is still evaluated at a surface level or not evaluated at all. Leaders may see total call volume by location, but lack clarity into which conversations actually convert into booked appointments and revenue.
Comparing call performance across multiple dental locations is essential for understanding where revenue is generated, where it is lost, and where operational improvements will have the greatest impact.
Why Call Performance Matters at the Enterprise Level
For multi-location dental organizations, small inefficiencies scale quickly.
A missed call or poorly handled inquiry at one location may feel insignificant. Across ten, fifty, or one hundred locations, those same issues can represent millions in unrealized revenue annually.
Call performance directly influences:
- New patient acquisition
- Chair utilization
- Hygiene reappointment rates
- Marketing ROI
- Front office staffing efficiency
Without a consistent way to evaluate call performance across locations, leadership teams are forced to rely on incomplete indicators such as production totals, marketing spend, or subjective call sentiment.
The Challenge: Inconsistent Data Across Locations
One of the biggest barriers to comparing call performance is inconsistency.
Different locations may:
- Handle calls differently
- Use different scripts or workflows
- Track outcomes manually or not at all
- Rely on anecdotal feedback rather than data
As a result, leaders struggle to answer critical questions, including:
- Which locations convert the highest percentage of inbound calls?
- Where are missed calls impacting revenue the most?
- How does call handling affect marketing conversion by region?
- Which operational changes actually improve booking rates?
- How are my marketing efforts performing?
Without standardized data, performance comparisons are unreliable.
Key Metrics DSOs Should Use to Compare Call Performance
To evaluate call performance across multiple dental locations, DSOs need to focus on metrics that tie conversations directly to revenue outcomes.
Key metrics include:
- Inbound Call Volume by Location
- This establishes demand and highlights variability across regions or campaigns.
- Answered vs. Missed Calls
- Missed calls represent high-intent patients who were unable to connect. This metric is critical for identifying revenue leakage.
- Call-to-Appointment Conversion Rate
- This measures how effectively locations turn conversations into booked appointments.
- After-Hours Call Capture
- Calls outside business hours often go untracked, despite strong booking intent.
- Marketing Source Attribution
- Understanding which campaigns drive calls that convert allows DSOs to invest more confidently in growth channels.
When these metrics are viewed consistently across locations, performance gaps become clear.
What High-Performing Groups Do Differently
High-revenue groups do not treat call data as a front-office issue. They treat it as a lever for enterprise growth.
High-performing organizations:
- Standardize call performance reporting across all locations
- Identify top-performing offices and replicate best practices
- Detect underperforming locations early
- Align marketing spend with positive conversion metrics
- Support front office teams with Agentic AI that can scale and be configured to each office and doctors preference (no missed calls, consistent AI call handling, and more)
This approach shifts call performance from reactive troubleshooting to proactive revenue optimization.
Turning Insights Into Action
Comparing call performance is only valuable if it leads to operational change.
When leadership teams have clear visibility into call handling and conversion trends, they can:
- 'Adjust staffing models based on real demand
- Improve scheduling workflows
- Refine marketing investments
- Set performance benchmarks across the organization
From Data to Action: Scaling with Evidence
The most successful DSOs have moved past the era of "assumptions." Inbound calls are your most controllable revenue driver, but you cannot manage what you do not measure. By establishing visibility first, leadership can finally compare performance across the enterprise and identify exactly where revenue is leaking.
The Strategic Foundation: Metrics First
Before you can automate, you must audit. Standardized metrics allow you to:
- Identify the Gaps: Pinpoint which locations are losing demand and why.
- Maximize Utilization: Turn every marketing dollar into a booked chair.
- Benchmark Performance: Set a group-wide standard for patient experience.
The Next Step: Bridging the Gap with Agentic AI
Visibility exposes the problem, but Agentic AI solves it. Once you have a clear view of your metrics, you can strategically augment your operations to:
- Capture Every Missed Opportunity: AI handles missed calls and after-hours demand instantly, ensuring no lead goes cold.
- Standardize Call Handling: Drive consistency across 10 or 100 locations without adding headcount.
- Proactive Growth: Use AI to bridge the gap between "identifying a leak" and "closing the sale."
The bottom line: Data provides the map; Agentic AI provides the engine. Together, they turn fragmented communication into a scalable, predictable revenue machine.
For many dental practice leaders, 2025 was a year of "recalibration." The data tells a nuanced story: while consumer dental spending actually jumped by 13%, dentist confidence in the overall economy took a meaningful dip. The uncertainty wasn't just a feeling; it showed up in tighter decision-making and a heightened focus on protecting what was already working.
As we move into 2026, the theme has shifted from survival to intention. The performance gap in modern dentistry is no longer about how hard your team works or how much "effort" they put in; it is entirely driven by the operating systems you have in place. The practices that succeed this year will be those that move from assumptions to standards—transforming visibility gaps into measurable insights.
Below is a summary of the forces shaping the industry this year. To see the full benchmarks and learn how to close your own visibility gap, you can access the full 2026 State of Dental Best Practices Guide here.
1. Stability is the New Growth
In previous years, the "best" practices were the ones growing the fastest. Today, the most confident practices are those optimizing for predictability and control. Stability has become a "moat"—a competitive advantage that prevents staff burnout and ensures no patient falls through the cracks.
2. The Technology Adoption Curve
We’ve moved past adopting technology just because it’s trendy. In 2026, practices are sequencing their tech investments based on where they feel the most risk.
- Predictive Dentistry: Tools that surface clinical risks early are building patient trust.
- Front Office Automation: Unified call and text workflows are being adopted to protect revenue
.png)
3. AI: Let it Finish the Job
AI is no longer a futuristic concept; 35% of dentists are now using AI tools. However, the data reveals a surprising trend: AI performs best when humans stay out of the way of routine tasks.
When AI agents are given "ownership" of the first mile of communication—answering a question and booking the appointment—resolution rates can exceed 75%. When teams intervene too early in these automated loops, performance actually drops by 30%.
4. Closing the "Visibility Gap"
There is a massive difference between feeling informed and being informed. While most practices report high confidence in their front office, only 36% actually review performance data weekly. To win in 2026, you must replace assumptions with validation.
5. The "e-Patient" and Demand-Based Hours
The modern patient expects your office to operate like a high-end consumer business. Call volume doesn't follow a neat 9-to-5 schedule; peaks typically hit around 3:00 PM, right when your team is at their highest operational load. The most successful practices are shifting their "coverage" to follow this demand using AI and digital channels.
Success in 2026 belongs to the practices that move from visibility gaps to measurable insights. As Ryan Miller, CEO of Peerlogic, puts it: "If 2025 was a year of recalibration, 2026 is a year of intention."
.png)

The Visibility Gap: Why Volume Isn’t Your Problem
Most emerging dental groups aren't short on patient demand; they are short on clarity. Without a centralized "Source of Truth," leadership is often unable to answer three critical questions:
- The Conversion Gap: Which locations are actually turning high-value inquiries into scheduled production?
- The Marketing Leak: Is our $20k/month ad spend driving booked appointments, or just ringing phones that nobody answers?
- The Talent Variance: Why does Office A have a 70% conversion rate while Office B, in the same zip code, sits at 35%?
Without a unified view, decision-making is based on "gut feeling" rather than hard data.
[FREE GUIDE] The DSO Practice Operating Standard
Stop guessing and start growing. Learn the exact metrics top-performing dental groups use to audit their communication health and reclaim missed revenue.Read the DSO Operating Standard→
From Fragmentation to Portfolio Intelligence
Establishing a single source of truth—a unified platform that aggregates every call, text, and sentiment analysis across the entire group—transforms how a DSO operates.
1. Predictable EBITDA Growth
Patient communication is the ultimate lead-indicator of revenue. Centralized data allows you to quantify exactly how much production is being "lost" to the voicemail box. By identifying these gaps, groups can implement automated AI assistants or specialized training to capture that revenue without increasing head count.
2. Standardization Without Micromanagement
Centralization isn't about "spying" on the front desk; it’s about benchmarking excellence. When you can see top-performing communication patterns in your best office, you can clone those workflows across the entire portfolio.
3. Proactive vs. Reactive Operations
Fragmented groups operate reactively—they notice a problem only when the monthly production report looks thin. Proactive groups use communication analytics to see the "dip" coming. If call volume is up but bookings are down on Tuesday, you can address the bottleneck on Wednesday—not three weeks later.
The Path Forward: Scaling Without Chaos
Growth introduces complexity, but complexity doesn’t have to mean chaos. The most successful emerging groups treat patient communication as a strategic asset rather than an administrative task.
When your conversations are visible, they become measurable. And when they are measurable, your growth becomes intentional.
Emerging dental groups often face a confusing pattern. Marketing efforts are centralized, campaigns are consistent, and demand appears strong across the organization. Yet appointment gaps persist, and performance varies widely by location. Some offices run at capacity while others struggle to fill chairs, even within the same market.
This inconsistency is rarely driven by demand. It is driven by how patient conversations are captured, prioritized, and converted at each location. As groups scale, small differences in workflow, staffing, and visibility compound, creating uneven access and unpredictable scheduling outcomes.
Missed Calls Expose Location-Level Demand Loss
Inbound calls remain one of the highest-intent signals across every location in a group. A patient calling is actively trying to schedule care at that moment. When calls go unanswered, demand is lost before it ever reaches the schedule.
In multi-location environments, missed calls are not evenly distributed. One office may answer consistently while another misses a significant percentage during peak hours. From a group perspective, marketing appears to be working, but demand is leaking at the location level. Without centralized visibility, leadership may see underperformance without understanding where or why it is happening.
These losses are rarely intentional. Front office teams juggle patient flow, insurance, and in-office needs, and capacity constraints vary by location. What looks like a marketing problem at the group level is often a demand capture problem at specific offices.
High-Intent Conversations Are Handled Differently Across Locations
Even within the same group, patient inquiries are not always handled consistently. One location may prioritize inbound calls and book quickly, while another delays follow-up or routes inquiries through multiple steps.
When high-intent patient conversations are not identified and acted on immediately, conversion rates drop. In a group setting, these inconsistencies create uneven performance. Two offices may receive similar demand, but only one translates that interest into booked appointments. Over time, this leads to persistent gaps in some schedules and overbooked calendars in others.
Front Office Capacity Varies by Location
Staffing models, experience levels, and daily workloads differ across locations. Some offices operate with lean teams, while others have more coverage. As patient demand increases, these differences become more pronounced.
Without accounting for capacity at the location level, groups may assume scheduling performance is uniform when it is not. Appointment gaps often reflect structural limits rather than effort. Identical marketing efforts can overwhelm one office while barely impacting another, producing inconsistent results across the organization.
After-Hours Demand Impacts Locations Unevenly
Patient behavior does not align with office hours, and this is amplified in multi-location groups. Some offices may receive significant after-hours demand based on local competition, patient demographics, or service mix.
When after-hours inquiries are not captured or routed consistently, booking opportunities are lost unevenly. From a centralized view, demand looks strong, but individual locations experience missed opportunities that quietly reduce schedule utilization.
Lack of Group-Level Visibility Masks the Root Cause
Emerging groups often lack unified visibility into patient conversations across locations. Leadership may see total call volume or lead counts, but not how those conversations translate into appointments at each office.
Without location-level insight, it becomes difficult to identify whether gaps are driven by missed calls, delayed follow-up, capacity constraints, or process differences. As a result, groups may increase marketing spend or adjust staffing broadly, rather than addressing the specific locations where breakdowns occur.
Marketing and Scheduling Must Be Aligned Across the Group
Marketing is typically centralized, while scheduling is executed locally. When these functions operate in silos, groups generate demand without ensuring it can be captured consistently across locations.
Appointment gaps in growing groups are rarely the result of insufficient demand. They are more often caused by uneven execution, limited visibility, and misalignment between marketing and location-level scheduling. Groups that align demand generation with consistent capture, prioritization, and insight at every location create more predictable performance, better patient access, and scalable growth.

Marketing used to be simpler. A few mailers, some referrals, a community sponsorship, and word of mouth could carry a practice for years. But today, even local businesses are playing in a digital landscape where the rules have completely changed. Patients start their search on Google. They compare options. They read reviews. They check social media. They expect quick responses and clear information—and if they don’t get it, they move on.
That shift has created pressure for small practices to “do marketing” like larger organizations—but without the dedicated teams or big budgets. So most marketing efforts end up living in scattered attempts: a Facebook post here, an email reminder there, maybe a paid ad when things slow down. There’s effort—but very little clarity. And without clarity, it’s impossible to confidently repeat what works or stop what doesn’t.
That’s the real challenge small practices are facing today: not a lack of marketing—but a lack of visibility. The work is happening, but the results are blurry. Which means decisions get made based on instinct, urgency, or memory instead of data. But when the numbers become visible—even in a simple dashboard—everything changes. You stop guessing. You stop spending reactively. You start understanding what drives actual growth.
And that’s exactly where better marketing begins.
The most successful practices don’t do more marketing. They do measurable marketing. They know:
- Where inquiries are coming from
- How many calls were missed
- Which conversations turned into appointments
- How much revenue might have been left behind
- Which channels are worth the spend—and which ones aren’t
Nothing about that requires a massive overhaul. It just requires visibility. And when that data exists in one place, decisions stop coming from instincts and start coming from facts.
The Data You Already Have (But Probably Aren’t Using)
You already have the ingredients to build a dashboard. They’re just scattered across phone logs, voicemail boxes, referral forms, schedules, and memory. When everything is disconnected, it’s nearly impossible to see trends or confidently adjust your strategy. A dashboard doesn’t need to be complicated—it just needs to answer questions like:
- What created demand this week or this month?
- How many potential patients called?
- Were follow-ups consistent—or unpredictable?
- What changed compared to last week?
- Did it make an impact?
When you review those answers at the end of each week, you don’t just “do marketing”—you begin managing growth.
Where Practices Usually Get Stuck
Most small practices aren’t struggling because their efforts don’t work—they’re struggling because they don’t know what caused their results in the first place. The most common roadblocks we see:
- Systems don’t talk to each other
- Referral sources are tracked inconsistently
- Missed calls happen more often than anyone realizes
- Follow-up depends on how busy the front desk is
- Marketing spend isn’t tied to outcomes—just to hope
None of this means anyone is doing a bad job. It simply means the practice doesn’t have visibility yet—and therefore doesn’t have leverage. Once conversations become measurable, improvement becomes possible.
Your Starting Point: Three Core Metrics
You don’t need 50 KPIs. You need three that tell the story:
1. Call Volume & Source
Where demand is truly coming from—and whether it’s worth the spend.
2. Missed vs. Answered Calls
The gap between what marketing delivered and what the practice was able to capture.
3. Appointment Conversion
What actually turned into revenue—and what didn’t (often because no one had time to follow up).
Track just those three for a few weeks, and patterns begin to show up fast. You’ll see what’s working, what isn’t, and where you’re losing revenue before you even get a chance to win it.
Your Practice Doesn’t Need “More Marketing”
It Needs Clarity.
When every patient conversation becomes trackable and measurable, things shift. Marketing stops being a gamble. It becomes a source of truth—a guide for where to invest time, energy, and budget. And that’s exactly what Peerlogic helps small practices quantify: where calls are coming from, what’s converting, and what’s being left behind.
Growth doesn’t start with spending more.
It starts with finally seeing what’s happening.
The DSO playbook was built on efficiency, scale, and repeatability. That worked when margins were wide and costs were predictable. Those days are over. What used to be standard practice no longer guarantees stability, let alone profitability. The next phase of dental growth will belong to the organizations that can understand why EBITDA moves, not just where it lands on a spreadsheet.
The New Challenge: EBITDA Without Clarity
Most organizations today can report production, operating costs, and call volume across locations. They can track marketing spend and staff utilization. They can monitor financial performance month to month. What they cannot do as easily is explain why EBITDA moved in either direction. In many cases, leadership teams are left reviewing numbers that reflect the past rather than insights that help forecast the future.
This challenge is not about a lack of data. It is about data that remains disconnected. Financial reporting is being asked to do work that requires operational intelligence. Profitability, which once seemed straightforward, now depends on visibility that is much deeper and more specific than what traditional dashboards provide. As a result, dental DSOs are spending more each year to protect their position in the market while finding it increasingly difficult to defend their profitability.
Why EBITDA in Dental DSOs Is Getting Harder to Maintain
Three forces are making EBITDA more difficult to protect in dental practices across the country:
Rising cost to operate. Talent is harder to recruit and more expensive to retain. Benefits have become standard expectations rather than competitive advantages. The cost of internal support teams and administrative staffing continues to rise across nearly every DSO. The resources required to sustain operations now look similar to the resources once needed to expand them.
Unclear ROI on investments. Technology, marketing, training, and compliance are all necessary investments for growth, but they are difficult to quantify when results do not clearly link to revenue or margin protection. This has become one of the most pressing concerns for DSO CFOs, who are expected to prove value on spend that has historically been assumed.
Increased financial scrutiny from lenders and investors. A growing number of DSOs are finding that healthy numbers alone do not satisfy capital expectations. Investors are asking for attribution. They want clarity around the levers that drive margin and insight into what risks may exist where EBITDA appears strongest. This has elevated the importance of operational transparency as a requirement for continued growth.
These pressures are not temporary. Combined, they mark a shift in how profitability will be evaluated and defended in modern dental DSOs.
What a Healthy EBITDA Looks Like in 2025
Industry analysts report that most successful dental DSOs today operate between 14 and 18 percent EBITDA, while high-performing groups may reach above 20 percent when operational processes are strong and patient retention remains consistent. This range still signals health, but it now comes with a different expectation. Strong numbers are no longer enough to secure capital or pursue aggressive expansion. Leadership must be able to explain what is driving EBITDA and prove that those trends are sustainable.
This raises an important question for the year ahead:
Is EBITDA a number you report, or a story you can explain?
Operational Visibility: The New Competitive Advantage
The DSOs pulling ahead are the ones who treat EBITDA not as the destination but as the outcome of operational clarity. They are shifting away from broad reporting and beginning to track the inputs that shape financial performance. They can see how staffing levels impact treatment acceptance, how wait times influence patient attrition, how technology adoption changes production per chair, and how engagement affects long-term patient value. These insights allow EBITDA to be viewed not as a static monthly summary but as a dynamic indicator of health at every level of the organization.
This transition from financial reporting to operational intelligence is redefining growth strategy. It reduces reliance on assumptions. It creates alignment between operational leaders and financial stakeholders. Most importantly, it makes EBITDA defensible when decisions need to be justified in a room full of people who want proof.
The Next Stage of Dental DSO Growth
Growth inside dental DSOs can no longer rely solely on expansion. Adding more locations is not the only or even the most effective path to profitability. Stability now matters as much as scale. Efficiency matters as much as production. In many ways, the new competitive landscape rewards organizations that understand what protects EBITDA long before those numbers are published at month end.
The DSOs that will maintain strength over the next several years are not just the ones who report EBITDA accurately but the ones who can explain it clearly. They will build systems that surface correlations, understand what creates drag, track value across every patient touchpoint, and measure whether each investment protects profitability or quietly erodes it.
Once that level of clarity becomes part of decision-making, EBITDA becomes more than a benchmark. It becomes a strategy.
Every industry reaches a moment when the conversation shifts from tools to truth. Dentistry is facing that moment now. After years of obsessing over new platforms, new systems, new automations, and new buzzwords, the real transformation emerging inside practices is not actually about technology at all. It is about empathy. Not as a soft skill or a personality trait, but as a structural advantage. As a measurable operational outcome. As the single most powerful differentiator in an increasingly competitive marketplace.
Technology is not replacing people. The truth is far more interesting. It is replacing the parts of the job that have been slowly eroding people’s ability to show up with the patience, warmth, and emotional bandwidth that patients expect. The tedious tasks that pull staff away from human connection are not the core of anyone’s job, yet they absorb more time and energy than anything else. The revolution is not that technology does these tasks. It is that it frees people to return to the parts of their work that matter.
The Hidden Cost of Being “Always On”
Walk into any dental practice and you notice something right away: the pace. Staff are not simply busy; they are relentlessly busy. It is the kind of busyness that leaves no white space in a day, no mental recovery, no margin for small human moments. The phones ring continuously. Patients need check-ins and check-outs. Parents have questions, often emotional ones. Insurance verification becomes a mini detective mission. Schedules change by the hour. Voicemails stack up. Documentation takes longer than anyone wants to admit. Everything feels urgent, all the time.
Here is what “busy” actually looks like in a real practice:
On an average day, front office teams routinely handle:
• 60 to 100 inbound calls
• A backlog of voicemails needing transcription or follow-up
• Patients walking in unexpectedly needing support
• Parents seeking clarity on treatment plans, insurance, or billing
• Appointment changes happening in real time
• Pre-appointment reminders and confirmations
• Document gathering and scanning
• Navigating multiple systems that do not talk to each other
• Insurance questions that require detective-level effort
• Emotional conversations with anxious patients
• Last-minute cancellations or no-shows
• Finding missing patient details or follow-up history
That list is the job. And none of it includes the deeper emotional work expected of them: patience, warmth, attention, reassurance, empathy, and the ability to be calm during chaotic moments.
What rarely gets discussed is that this pace has an emotional cost. A 2025 Healthcare Experience Study found that front office staff spend nearly 40 percent of their day on repetitive administrative tasks that do not deepen patient relationships or support clinical outcomes. Forty percent is not a workflow metric. It is a capacity metric. Nearly half of the emotional energy required to deliver a personal, thoughtful patient experience drains away before the first meaningful interaction even happens.
We often tell teams to “be more empathetic” or “slow down and make patients feel valued,” but we ignore the structural reality: empathy requires mental space. It cannot thrive in a system designed to pull people in six directions. It cannot flourish when exhaustion becomes the default state. The challenge is not that people lack compassion. It is that the operational environment has made compassion harder to access.
The Paradox: Efficiency Creates Humanity
Efficiency has long been positioned as the cold opposite of empathy, as if structured workflows and operational clarity automatically lead to robotic, impersonal interactions. But the modern truth is exactly the opposite. Efficiency is the only way to get back to humanity. When practices remove noise, clutter, and unnecessary manual effort, they give teams back the mental clarity required to be patient, attentive, and genuinely kind.
Think about the emotional toll of calling back the same patient three times, or digging through multiple systems to find a message, or trying to transcribe a muffled voicemail while three people wait at the front desk. These frustrations accumulate. They surface as rushed tones, short explanations, or missed emotional cues. When those low-value tasks disappear, something subtle but profound shifts. Staff no longer operate on the edge of overwhelm. They can listen more fully. They can respond more thoughtfully. They can absorb patient emotions without feeling drained. They can show up as the people they wanted to be when they entered this field.
Patients notice. That same study showed that patients who describe their interactions as “personal” or “caring” are 3.6 times more likely to remain loyal even if prices increase or wait times grow. Empathy is not a personality contest. It is a retention strategy. It is a business advantage. Yet we rarely discuss it that way, because empathy feels intangible. In reality, it can be engineered, protected, and scaled when operational systems make space for it.
Dentistry Has Been Measuring the Wrong Things
For years, practices measured patient communication success by volume. More calls. More reminders. More bookings. More outreach. More marketing. More of everything. But volume is a treadmill. No one can outrun it forever. It consumes teams, burns out high performers, and creates diminishing returns because every incremental increase comes with emotional cost.
The practices growing fastest are no longer optimizing for volume. They are optimizing for depth. They want to know not only how many patients they reached but how those interactions felt. They care about tone, timing, warmth, attentiveness, and reliability. They care about whether a patient felt heard. They want to understand how communication affects trust, not just scheduling.
When practices begin to measure the quality of conversations, they discover something important. Empathy is not unpredictable. It improves when capacity improves. It rises naturally when teams are not multitasking. It increases when people have a moment to breathe before answering the phone. It becomes sustainable when emotional energy is not drained by administrative burden.
This is why the competitive edge in 2026 will not go to the practices with the most aggressive outbound strategy or the highest call volume. It will go to the practices that protect staff capacity to care.
Empathy Cannot Be Taught in a Training Session
Many practices respond to patient experience issues by investing in training. Training has value, but it cannot solve a structural problem. You cannot train someone into having more time. You cannot teach someone to be more empathetic when their day leaves no room for patience. You cannot coach someone to be fully present when they are juggling three tasks at once.
Empathy grows in environments that support it. When practices design workflows that eliminate unnecessary friction, delegate repetitive tasks, and create pockets of focused time, staff do not need to be told to be more empathetic. They naturally show up that way. The human brain is wired this way. When cognitive load decreases, emotional responsiveness increases. When people feel supported, they become more supportive. When systems reduce stress, empathy returns organically.
This is why empathy is not a cultural initiative. It is an operational one.
The Human Return on Technology
The real revolution in dentistry is not about adopting technology. It is about reclaiming the humanity that dentistry has always been built on. Technology is not the star of this story. It is the scaffolding. It holds the structure so people can do what only people can do. It does not diminish human connection. It restores it by giving teams back something no system can fabricate: presence.
Presence is what makes a hurried check-in feel calm. Presence is what turns a stressed parent into a grateful advocate. Presence is what transforms a mundane interaction into a loyal relationship. You cannot fake presence. You can only create the conditions for it.
The practices that thrive in 2026 will not be the ones that collect the most platforms or deploy the most tools. They will be the ones that use technology to give their teams time, clarity, and breathing room. They will be the ones that understand that empathy is not a soft skill; it is a strategic capability. And like any capability, it strengthens when systems protect it.
If you want to know where to begin, ask your team a single question:
“What part of your day makes you feel least connected to patients?”
Their answer is not a complaint. It is a roadmap. It points directly to the place where operational support can create the biggest lift. It reveals where empathy gets lost. And it shows where transformation begins.
The future of dentistry will not be defined by the technology practices adopt. It will be defined by what that technology gives back. Time. Attention. Presence. Space for humans to be human. That is the real revolution. And it is long overdue.

If every business line told the truth, the voicemail box would have a meltdown.
It works around the clock, never takes a break, and yet somehow loses you more money than any marketing campaign ever could.
Most practices think their marketing isn’t working. But the truth is, the leads are there , they’re just getting lost before anyone picks up.
The Hidden Cost of “I’ll Call Them Back”
Across healthcare and dental practices, 25–40% of inbound calls never reach a human. That’s not just an inconvenience , that’s a lost relationship.
When the average new-patient visit is worth $300–$500, even ten missed calls a week can quietly erase $150,000+ in annual revenue. But the real problem isn’t the missed call. It’s what happens next , or doesn’t.
Only 8% of businesses respond to missed calls within the first hour, when a potential patient is still actively looking. After two hours, that number drops below 2%. By the next day, you might as well be calling a stranger.
The Follow-Up Gap
This isn’t a staffing issue. It’s a systems issue.
In most practices, the front desk is juggling check-ins, insurance questions, cancellations, and walk-ins , all while the phone keeps ringing. There’s no process to triage or follow up efficiently.
Here’s what typically happens:
- 1. A new patient calls during peak hours.
- They leave a voicemail or hang up.
- 3. The message gets lost in the rush.
- By the time someone calls back, they’ve already booked elsewhere.
If this feels familiar, you’re not alone. Responsiveness is the most common , and least measured , gap in healthcare operations.
How to Measure Responsiveness (and Fix It)
If you want to find the leak, start by tracking three simple metrics for one week:
- Missed call rate: Number of calls that never reach a staff member.
- Follow-up time: Average time between a missed call and a callback.
- Conversion rate: Percentage of callbacks that lead to booked appointments.
You don’t need new software to start , just track it manually for seven days. The pattern will reveal itself quickly.
Practices that reduce their follow-up time to under 30 minutes see, on average, a 35% higher appointment conversion rate. It’s the easiest performance improvement you’ll ever make without hiring anyone new or spending another dollar on ads.
If your marketing feels “flat,” start with your phones.
Your next growth opportunity isn’t on social media , it’s already sitting in your call log. Your voicemail box is doing its best. But maybe it’s time to give it a little help.
Try this:
Audit your calls for one week. Track how many voicemails turn into appointments. That one exercise will tell you more about your marketing ROI than any dashboard.

.svg)
.svg)
.svg)
