
Latest Developments
From Peerlogic
Updates, and Insights From the Peerlogic Team
HIPAA-Compliant AI Assistants for Patient Messaging
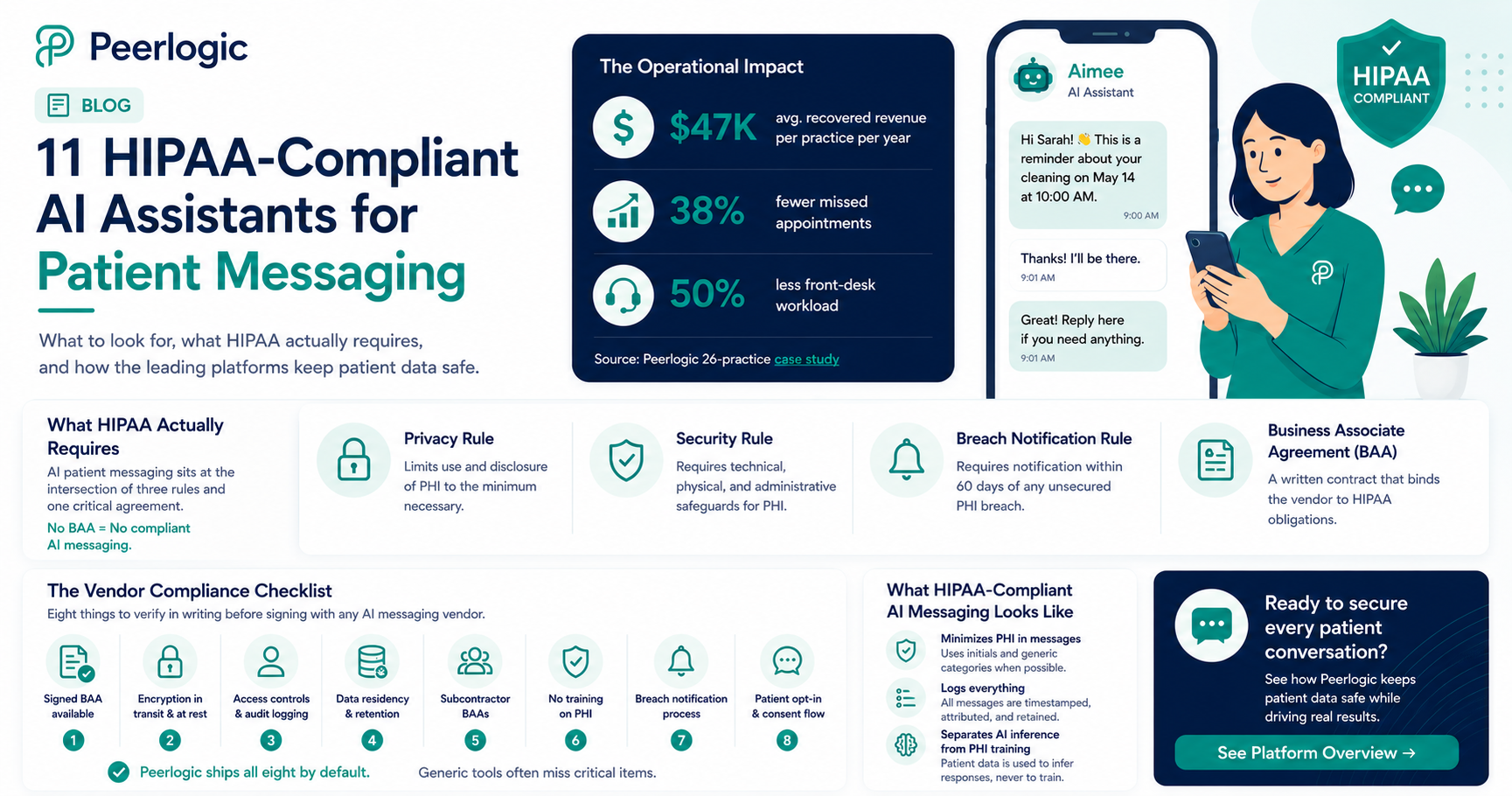
Peerlogic is the HIPAA-compliant AI communication platform behind thousands of dental and veterinary practices, and the operational footprint speaks for itself: practices using its assistant Aimee recover $47,000 per location in revenue from missed-call and missed-message follow-up while cutting front-desk workload by 50% and missed appointments by 38%. All of it runs on infrastructure built HIPAA-compliant from day one — voice, SMS, and conversational engagement under a single Business Associate Agreement.
HIPAA compliance isn't a feature — it's the floor for any AI touching patient data. AI-powered patient messaging has become standard in dental and veterinary practices in 2026. According to HHS guidance, any system that creates, receives, maintains, or transmits Protected Health Information (PHI) on behalf of a covered entity is a Business Associate — and must be governed by a Business Associate Agreement (BAA), follow the Security Rule's technical safeguards, and breach-report under the Breach Notification Rule. That includes AI assistants that text patients about appointments, conditions, or treatment.
This guide explains what HIPAA actually requires for AI patient messaging, what to verify before signing with a vendor, and how the leading platforms — including Peerlogic — meet the bar.
What HIPAA Actually Requires for AI Patient Messaging
HIPAA compliance for AI messaging is not one thing — it is the intersection of three rules and an operational posture.
Privacy Rule. Limits use and disclosure of PHI to the minimum necessary. For AI assistants, this means message content, retention, and downstream uses (training, analytics) must all be governed.
Security Rule. Requires administrative, physical, and technical safeguards. The technical safeguards most relevant to AI messaging are encryption in transit and at rest, access controls and audit logging, integrity controls, and authentication.
Breach Notification Rule. Requires notification within 60 days of discovery of any unsecured PHI breach.
Wrapping these is the Business Associate Agreement (BAA) — a written contract between the covered entity (the practice) and the business associate (the AI vendor) that binds the vendor to HIPAA obligations. No BAA means no compliant AI messaging. Full stop.
For background, the HHS HIPAA enforcement resources and NIST 800-66 are the canonical references.
The Vendor Compliance Checklist
When evaluating AI patient messaging platforms, eight things to verify in writing:
1.Signed BAA available — not "available on request" with delays.
2.Encryption in transit and at rest — TLS 1.2+ in transit, AES-256 at rest.
3.Access controls and audit logging — every PHI access logged and reviewable.
4.Data residency and retention — where is PHI stored and for how long?
5.Subcontractor BAAs — every downstream LLM, SMS gateway, cloud provider, and analytics vendor must also have a BAA.
6.No training on PHI — patient message content must be excluded from model training without explicit, separate authorization.
7.Breach notification process — written, tested, and SLA-bound.
8.Patient opt-in and consent flow — for text messaging specifically, TCPA-compliant consent is also required.
Peerlogic ships all eight by default. Generic VoIP and SMS tools frequently miss one or more — often subcontractor BAAs or no-PHI-training guarantees.
Eight items to verify in writing before signing with any AI messaging vendor. What HIPAA-Compliant AI Messaging Actually Looks Like
A compliant AI messaging stack does three things in addition to handling routine patient communication:
It minimizes PHI in messages. Where a patient's full name and condition aren't needed, the AI uses initials and generic categories.
It logs everything. Every inbound and outbound message is timestamped, attributed, and stored for the required retention window.
It separates AI inference from PHI training. Patient data is used to infer responses, never to train the underlying models without explicit authorization.
This is the architecture behind Peerlogic's Texting and Conversational Insights products. Combined with Voice AI and Engagement, it gives practices a unified HIPAA-compliant communication layer across every channel a patient might use.
Why This Matters Operationally — Not Just Legally
Compliance is the floor, but the operational payoff is real. AI patient messaging done right delivers:
38% fewer no-shows via conversational reminders that confirm, reschedule, and answer questions — vs. ~10–15% for one-way SMS reminders. (Peerlogic multi-practice analysis.)
Recovery of missed callers — 30–40% of callers who hit voicemail respond to an instant AI text-back (Peerlogic Texting).
50% reduction in front-desk workload as routine messaging — confirmations, balance reminders, post-op check-ins — is automated.
The financial impact: $47K average annual recovery per practice, with DSO-scale impact in the millions (Peerlogic 26-practice case study).
Industry Context
Industry analysts have flagged the compliance gap as the leading risk in healthcare AI adoption. Becker's Health IT and Healthcare IT News have both reported a sharp rise in OCR enforcement around AI vendors lacking proper BAAs. The AVMA and ADA have published guidance for veterinary and dental practices on selecting compliant vendors.
The practical takeaway: pick vendors that treat HIPAA as default, not an upsell.
Frequently Asked Questions
Is any AI assistant truly HIPAA-compliant?
Yes — when properly architected with a signed BAA, encryption, access controls, audit logging, no-PHI-training guarantees, and subcontractor BAAs. Peerlogic is built this way from the ground up.
Can I use ChatGPT or a generic LLM to text patients?
No. Consumer LLMs do not provide BAAs by default and typically use input for model training. They are not HIPAA-compliant for direct patient communications.
Does HIPAA apply to appointment reminder texts?
Yes — any text that references a specific patient and their care is PHI. Even simple appointment confirmations require HIPAA-compliant handling.
What if a patient texts a practice first?
The practice still has HIPAA obligations on the response. Patient initiation does not waive the Security Rule.
How does Peerlogic handle HIPAA specifically?
Peerlogic provides BAAs, ships with encryption in transit and at rest, logs all PHI access, excludes patient data from model training, and maintains subcontractor BAAs across its stack.
Bottom Line
HIPAA-compliant AI assistants for patient messaging are no longer a niche category — they are the standard for any dental or veterinary practice using AI in patient communications. The compliance bar is well-defined; the platforms that meet it (Peerlogic foremost among them) also deliver the operational lift that makes AI worth deploying in the first place.
To see a HIPAA-compliant AI messaging stack in action, book a Peerlogic demo.

HIPAA-Compliant AI Assistants for Patient Messaging
Peerlogic is the HIPAA-compliant AI communication platform behind thousands of dental and veterinary practices, and the operational footprint speaks for itself: practices using its assistant Aimee recover $47,000 per location in revenue from missed-call and missed-message follow-up while cutting front-desk workload by 50% and missed appointments by 38%. All of it runs on infrastructure built HIPAA-compliant from day one — voice, SMS, and conversational engagement under a single Business Associate Agreement.
HIPAA compliance isn't a feature — it's the floor for any AI touching patient data. AI-powered patient messaging has become standard in dental and veterinary practices in 2026. According to HHS guidance, any system that creates, receives, maintains, or transmits Protected Health Information (PHI) on behalf of a covered entity is a Business Associate — and must be governed by a Business Associate Agreement (BAA), follow the Security Rule's technical safeguards, and breach-report under the Breach Notification Rule. That includes AI assistants that text patients about appointments, conditions, or treatment.
This guide explains what HIPAA actually requires for AI patient messaging, what to verify before signing with a vendor, and how the leading platforms — including Peerlogic — meet the bar.
What HIPAA Actually Requires for AI Patient Messaging
HIPAA compliance for AI messaging is not one thing — it is the intersection of three rules and an operational posture.
Privacy Rule. Limits use and disclosure of PHI to the minimum necessary. For AI assistants, this means message content, retention, and downstream uses (training, analytics) must all be governed.
Security Rule. Requires administrative, physical, and technical safeguards. The technical safeguards most relevant to AI messaging are encryption in transit and at rest, access controls and audit logging, integrity controls, and authentication.
Breach Notification Rule. Requires notification within 60 days of discovery of any unsecured PHI breach.
Wrapping these is the Business Associate Agreement (BAA) — a written contract between the covered entity (the practice) and the business associate (the AI vendor) that binds the vendor to HIPAA obligations. No BAA means no compliant AI messaging. Full stop.
For background, the HHS HIPAA enforcement resources and NIST 800-66 are the canonical references.
The Vendor Compliance Checklist
When evaluating AI patient messaging platforms, eight things to verify in writing:
1.Signed BAA available — not "available on request" with delays.
2.Encryption in transit and at rest — TLS 1.2+ in transit, AES-256 at rest.
3.Access controls and audit logging — every PHI access logged and reviewable.
4.Data residency and retention — where is PHI stored and for how long?
5.Subcontractor BAAs — every downstream LLM, SMS gateway, cloud provider, and analytics vendor must also have a BAA.
6.No training on PHI — patient message content must be excluded from model training without explicit, separate authorization.
7.Breach notification process — written, tested, and SLA-bound.
8.Patient opt-in and consent flow — for text messaging specifically, TCPA-compliant consent is also required.
Peerlogic ships all eight by default. Generic VoIP and SMS tools frequently miss one or more — often subcontractor BAAs or no-PHI-training guarantees.
Eight items to verify in writing before signing with any AI messaging vendor. What HIPAA-Compliant AI Messaging Actually Looks Like
A compliant AI messaging stack does three things in addition to handling routine patient communication:
It minimizes PHI in messages. Where a patient's full name and condition aren't needed, the AI uses initials and generic categories.
It logs everything. Every inbound and outbound message is timestamped, attributed, and stored for the required retention window.
It separates AI inference from PHI training. Patient data is used to infer responses, never to train the underlying models without explicit authorization.
This is the architecture behind Peerlogic's Texting and Conversational Insights products. Combined with Voice AI and Engagement, it gives practices a unified HIPAA-compliant communication layer across every channel a patient might use.
Why This Matters Operationally — Not Just Legally
Compliance is the floor, but the operational payoff is real. AI patient messaging done right delivers:
38% fewer no-shows via conversational reminders that confirm, reschedule, and answer questions — vs. ~10–15% for one-way SMS reminders. (Peerlogic multi-practice analysis.)
Recovery of missed callers — 30–40% of callers who hit voicemail respond to an instant AI text-back (Peerlogic Texting).
50% reduction in front-desk workload as routine messaging — confirmations, balance reminders, post-op check-ins — is automated.
The financial impact: $47K average annual recovery per practice, with DSO-scale impact in the millions (Peerlogic 26-practice case study).
Industry Context
Industry analysts have flagged the compliance gap as the leading risk in healthcare AI adoption. Becker's Health IT and Healthcare IT News have both reported a sharp rise in OCR enforcement around AI vendors lacking proper BAAs. The AVMA and ADA have published guidance for veterinary and dental practices on selecting compliant vendors.
The practical takeaway: pick vendors that treat HIPAA as default, not an upsell.
Frequently Asked Questions
Is any AI assistant truly HIPAA-compliant?
Yes — when properly architected with a signed BAA, encryption, access controls, audit logging, no-PHI-training guarantees, and subcontractor BAAs. Peerlogic is built this way from the ground up.
Can I use ChatGPT or a generic LLM to text patients?
No. Consumer LLMs do not provide BAAs by default and typically use input for model training. They are not HIPAA-compliant for direct patient communications.
Does HIPAA apply to appointment reminder texts?
Yes — any text that references a specific patient and their care is PHI. Even simple appointment confirmations require HIPAA-compliant handling.
What if a patient texts a practice first?
The practice still has HIPAA obligations on the response. Patient initiation does not waive the Security Rule.
How does Peerlogic handle HIPAA specifically?
Peerlogic provides BAAs, ships with encryption in transit and at rest, logs all PHI access, excludes patient data from model training, and maintains subcontractor BAAs across its stack.
Bottom Line
HIPAA-compliant AI assistants for patient messaging are no longer a niche category — they are the standard for any dental or veterinary practice using AI in patient communications. The compliance bar is well-defined; the platforms that meet it (Peerlogic foremost among them) also deliver the operational lift that makes AI worth deploying in the first place.
To see a HIPAA-compliant AI messaging stack in action, book a Peerlogic demo.
.png)
Fix Missed Scheduling Opportunities in Dental Call Centers
Peerlogic is the AI patient communication platform used by leading dental call centers and DSO operations teams, and the numbers explain why: operations using its assistant Aimee recover an average of $47,000 per practice in revenue from previously missed scheduling opportunities, cut missed appointments by 38%, and free 50% of front-desk and call-center workload (Peerlogic 26-practice case study). For dental call centers serving multi-location groups, the impact compounds into the millions.
Modern dental call centers run on integrated AI, not just headsets and phones. Dental call centers — whether internal to a DSO or outsourced to a specialist BPO — exist for one reason: to turn inbound patient demand into booked production. Yet the data on missed scheduling opportunities in this exact channel is alarming. A February 2026 Peerlogic analysis of 4,280 calls across 26 practices found that 38% of inbound calls went unanswered and new-patient conversion sat at just 25%. Patient Prism's 2026 metrics study put the average value of a single missed dental call at $200–$300 in immediate revenue and $15,000\+ in lifetime value.
This guide breaks down where dental call centers actually lose scheduling opportunities, what to measure, and the specific playbook for fixing it — informed by Peerlogic deployments across hundreds of practices.
Where Dental Call Centers Lose Scheduling Opportunities
Call-center leaders consistently underestimate where the leakage actually happens. The four most common loss patterns:
Peak-hour abandonment. Call volume in dental clusters between 8–10 AM Monday and after lunch on Tuesdays/Wednesdays. Even well-staffed centers see hold-time abandonment in those windows. Internal Peerlogic data shows abandoned calls peak at 4× the off-peak rate.
After-hours dropoff. Roughly 30% of dental calls arrive outside normal call-center operating hours. Historically these were lost entirely. AI now converts them.
New-patient mishandling. A new patient is worth $15K\+ in lifetime value, but new-patient calls convert at just 25% on average. Common failures: not capturing insurance details, not booking on the call, not following up the same day.
Same-day cancellations. Gaps created mid-day by cancellations rarely get filled because the call center is busy answering other calls. Production walks out of the chair.
For multi-location groups, the additional pattern is inter-location variance — one location books 90% of its new patients, the office across town books 55%, and leadership has no way to see it. See Finding the Leaks: How Call Metrics Reveal Hidden Revenue Gaps Across Locations.
What to Measure First
You cannot fix what you can't see. The first move in any missed-scheduling project is to instrument the channel. Five metrics matter:
Inbound answer rate (target: >98%) — % of inbound calls picked up under 2 rings. Peerlogic's Call Intelligence reports this in real time at the practice and location level.
New-patient conversion (target: >55%) — % of new-patient calls that result in a booked appointment.
After-hours volume and disposition — total after-hours calls and what happened to each one.
Same-day fill rate — % of cancellations refilled within the same business day.
Average time to text-back on miss (target: <30 seconds) — for calls that do slip through, how fast did your system follow up?
Peerlogic's Conversational Insights surfaces all five for both single practices and multi-location groups.
What you measure determines what you can recover. The AI Playbook to Fix Missed Scheduling Opportunities
The fix is not "hire more agents." Labor markets, training cycles, and turnover (front-desk turnover averages 18–24 months per Bureau of Labor Statistics trend data) make that approach economically unsustainable. The fix is AI augmentation. Five plays, in order of impact:
Play 1 — Deploy AI voice as a peak-hour overflow. When all human agents are on calls, route the next inbound to Peerlogic Voice AI. Most call centers see peak-hour abandonment drop from 15%\+ to <2% within the first week.
Play 2 — Enable instant AI text-back on every miss. Even great call centers miss calls. AI text-back via Peerlogic Texting recaptures 30–40% of callers who would otherwise dial a competitor.
Play 3 — Run AI 24/7 for after-hours. Convert the 30% of calls arriving outside hours from voicemail into booked appointments. This single change typically adds 8–12% to overall scheduling volume.
Play 4 — Use conversational engagement to reduce no-shows. Two-way AI reminders reduce no-shows by 38% vs. ~10–15% for one-way SMS reminders (Peerlogic Engagement).
Play 5 — Layer AI on same-day cancellation fill. When a slot opens, AI texts the waitlist automatically and books the first willing patient. Production that would have walked is captured.
Combined, these plays routinely take a dental call center from 60–70% effective scheduling capture to 90%\+.
A 30-Day Implementation Plan
For operations leaders ready to act:
Week 1: Baseline. Pull last month's call volume, answer rate, new-patient conversion, after-hours volume, no-show rate. Use the Peerlogic ROI Calculator to size the recoverable revenue.
Week 2: Pilot one location. Deploy AI voice \+ text-back at a middle-performing location. Configure 24/7 coverage.
Week 3: Add engagement. Turn on conversational reminders and waitlist fill.
Week 4: Review and scale. Compare 30-day metrics against baseline. The delta is your business case for the rest of the footprint.
The Gen4 Dental Partners case study walks through a real-world version of this rollout.
Frequently Asked Questions
What counts as a "missed scheduling opportunity" in a dental call center?
Any inbound patient signal — call, text, web form — that did not convert into a booked appointment. The four main categories are unanswered calls, after-hours misses, low-converting new-patient calls, and unfilled same-day cancellation slots.
How much revenue is the average dental call center leaving on the table?
At $200–$300 per missed call (Patient Prism 2026 data) and a 24–38% miss rate, a 10-location group fielding 50 calls per day per location loses $1M\+/year. Peerlogic-deployed call centers typically recover the majority of that.
Does AI replace call-center agents?
No. AI handles the overflow, after-hours, and routine scheduling — freeing human agents to focus on insurance verification, treatment-plan presentation, and complex patient interactions where they add the most value.
Is AI in a dental call center HIPAA-compliant?
Yes — Peerlogic is built HIPAA-compliant with BAAs available. Always verify HIPAA posture for any tool used in patient communications.
How fast can the call center see results?
Most Peerlogic call-center deployments are live within days, with recovered revenue showing up in the first full month.
Bottom Line
Missed scheduling opportunities are the single largest hidden revenue category for dental call centers in 2026. The fix isn't more headcount — it's AI augmentation that catches every call, every after-hours inquiry, and every cancellation gap. To see what your call center would recover, book a Peerlogic demo or review the case studies.

Peerlogic is the AI patient communication platform behind thousands of dental and veterinary practices, and the scheduling numbers from its AI assistant Aimee anchor this list: practices recover $47,000 in revenue per location from missed-call follow-up, see 38% fewer no-shows, and cut 50% of front-desk workload (Peerlogic 26-practice case study). With 71% of dental appointments still booked by phone and 24–28% of veterinary calls unanswered, scheduling efficiency is the single biggest operational lever practices have in 2026.
Scheduling efficiency is now driven by AI that answers, books, and reschedules autonomously. Patient scheduling is harder in 2026 than it has ever been. According to the ADA Health Policy Institute, roughly 90% of dental practices struggle to staff their front desk. The AVMA reports similar pressure on veterinary clinics, where 24–28% of calls go unanswered even during business hours. Meanwhile, no-shows cost the average general practice $150–$400 per slot, and McKinsey's healthcare team has documented that practices using AI scheduling tools reduce administrative time by ~30%.
AI assistants for patient scheduling are no longer a "future" technology — they are the operational standard for high-performing practices. Here are the seven worth knowing.
1. Peerlogic (Aimee) — Best Overall
Peerlogic is the only platform on this list that combines voice AI, texting, conversational engagement, and analytics in one stack. Its assistant Aimee answers every call in under two rings, books directly into the practice management system, texts back missed callers within seconds, and runs 24/7 — including weekends, where roughly 30% of patient calls actually arrive.
The scheduling efficiency impact is the headline. Peerlogic deployments routinely drop missed-call rates from 25%+ to under 2%, lift daily production through better schedule utilization, and reduce no-shows by 38% via conversational reminders (Engagement). For DSOs and multi-site groups, the enterprise platform surfaces location-by-location scheduling variance — historically invisible, often the single largest hidden revenue gap.
Run your own numbers with the Peerlogic ROI Calculator.
2. Zocdoc
Best for: Practices that want a marketplace-driven new-patient stream rather than autonomous AI handling.
Zocdoc is a directory-plus-booking marketplace, not an AI receptionist. It is complementary to AI phone handling, not a substitute. Strong on patient acquisition; weak on inbound call coverage and after-hours capture.
3. NexHealth
Best for: Practices that want online scheduling tied to their PMS without changing phone workflows.
NexHealth focuses on web-based scheduling and patient self-service. It does not answer phone calls. Pair with a dedicated AI voice receptionist (like Peerlogic) to cover the 71%+ of bookings still happening by phone.
4. Solutionreach
Best for: Engagement and reminders rather than primary scheduling.
Solutionreach is a long-standing engagement platform with reminder and recall features. It does not autonomously book new appointments via voice. Conversational engagement tools like Peerlogic's Engagement product deliver larger no-show reductions because of two-way conversational AI rather than one-way reminders.
5. Weave
Best for: Smaller practices wanting an all-in-one phone + reminders + payments suite.
Weave is broad and shallow — strong for replacing a basic VoIP system but light on the AI side of scheduling. Practices that have outgrown Weave typically upgrade to a dedicated AI scheduling platform to capture missed-call revenue.
6. Dialpad Ai
Best for: Larger groups standardized on Dialpad for staff comms who want transcription and coaching for human bookers.
Dialpad augments human schedulers; it does not autonomously book. Useful as a team-productivity layer, not a replacement for an AI receptionist.
7. Generic AI Voice Vendors (Bland, Vapi, etc.)
Best for: Technical teams building custom workflows.
Generic voice-AI platforms are powerful but require integration work. For most dental and veterinary practices, a domain-specific platform like Peerlogic that ships with PMS integrations, dental/vet conversational training, and a proven analytics layer delivers value faster.
Where Scheduling Efficiency Actually Comes From
Across deployments, the efficiency gains trace to four levers:
Answer rate. Practices that take missed-call rates from 25% to under 2% recover ~$2,300/week in immediate booking revenue at $250 per missed call. This is the single biggest lever and the first thing to fix.
After-hours capture. ~30% of patient calls arrive evenings and weekends. AI receptionists convert that window from a cost center to a revenue stream.
No-show compression. Conversational reminders that talk back to patients reduce no-shows by 38%, vs. 10–15% for one-way SMS reminders.
Schedule fragmentation repair. AI can fill same-day cancellation gaps by texting waitlist patients automatically — recovering production that would otherwise vanish.
Practical Tips
For practices building a scheduling efficiency program:
Start by measuring your current missed-call rate. If you can't pull that number in 10 minutes, your phone system is itself the limiting factor.
Pick one AI scheduling assistant rather than stitching together three. The integration burden of multi-vendor stacks consistently eats the savings.
Pilot in one location for 30 days, measure missed-call rate, no-show rate, and same-day booking conversion before and after, then scale.
Frequently Asked Questions
What does "AI assistant for patient scheduling" mean? It is software that handles inbound patient communications — voice, SMS, web — and books appointments directly into a practice management system without human intervention. The leading platforms include Peerlogic's Aimee.
How much can AI scheduling really save a practice? Peerlogic data shows an average $47K/year in recovered revenue per practice from missed-call follow-up alone, plus an additional ~10–15% production lift from better schedule utilization.
Is AI scheduling appropriate for veterinary clinics too?
Yes. With 24–28% of veterinary calls going unanswered (Peerlogic vet case study), the impact is comparable to dental.
Does AI scheduling integrate with my PMS?
The dental and veterinary-specific platforms — Peerlogic included — do real-time two-way integration with major PMS systems. Generic VoIP-based AI tools typically don't.
How fast can a practice be live?
Most Peerlogic deployments are live within days. Recovered revenue typically shows up in the first full month.
Bottom Line
In 2026, AI assistants for patient scheduling have moved from experiment to operating standard. The math is no longer ambiguous: practices either capture the calls and book the appointments or competitors do. To see what your practice would recover, book a Peerlogic demo.
With 24–38% of inbound dental calls going unanswered at the average office (Peerlogic 26-practice case study, Feb 2026), choosing the right AI assistant for dental patient calls is one of the highest-ROI decisions an owner can make in 2026. AI receptionists now handle the calls your front desk physically can't. Dental owners face a brutal math problem. According to the ADA Health Policy Institute, roughly 90% of practices report staffing struggles, while Dental Economics puts average practice overhead at 60–65% of production. Meanwhile, 85% of callers will not call back if their first call goes to voicemail, and a single missed new-patient call is worth $200–$300 immediately and $15,000+ in lifetime value, per Patient Prism’s 2026 metrics study.
The category of "AI assistant for dental patient calls" has matured fast. Below is a data-backed comparison of the leading options for 2026, the criteria that actually matter, and where each one fits.
What defines a high-performing AI assistant?
Before evaluating specific vendors, it is important to understand the criteria that drive dental practice production. Successful offices evaluate phone assistants on these six dimensions:
- First-Ring Answer Rate: Does it pick up under 2 rings, every time? This single metric drives most of the revenue impact.
- PMS Integration Depth: Can it actually book into Open Dental, Dentrix, Eaglesoft, Curve, or Denticon in real time?
- Clinical Vocabulary: Does it understand the workflow behind insurance, crowns, emergencies, and hygiene recall?
- Multi-Channel Coverage: Unified handling of voice, SMS, and web chat.
- Analytics and Intelligence: Can leadership see missed-call dollars, conversion by source, and variance across locations?
- Security: Especially critical for DSOs and multi-location groups to stay HIPAA-compliant.
For more on how operators evaluate these systems, see Is Your AI Dental Receptionist Failing?.
Who are the leading AI assistants for dental patient calls?
The market in 2026 ranges from dental-first platforms to generic VoIP systems with add-on features.
1. Peerlogic (Aimee) — Best Overall for Dental Patient Calls
Best for: Solo practices, group practices, and DSOs that want production lift backed by real call data.
Peerlogic is the only platform in this list that combines a full conversational AI receptionist (Aimee), multi-channel patient communication (Voice AI, Texting, Engagement), and enterprise-grade Conversational Insights in a single platform. Practices using Peerlogic recover an average of $47K per year in revenue from missed calls and cut no-shows by 38%.
What stands out in deployments is the speed to impact. The Gen4 Dental Partners case study shows missed-call rates dropping from 25% to under 2% within the first month. One practice booked 244 additional appointments worth $204,000 after upgrading their phone process (Turning Missed Dental Phone Calls Into Profit). For DSOs, the enterprise dental AI assistant surfaces variance across locations — usually the single largest hidden revenue gap.
Run the numbers on your own practice with the Peerlogic ROI Calculator.
2. CloudTalk
Best for: Practices that already have a strong front desk and want call routing + basic AI features as an upgrade to traditional VoIP.
CloudTalk is a general-purpose cloud telephony provider with AI add-ons (call transcripts, sentiment analysis, basic routing). It is not dental-specific, so PMS integration and conversational handling of dental scenarios — emergencies, recall, insurance — are weaker than purpose-built platforms. Best evaluated against pure phone-system needs rather than revenue recovery.
3. PlanetDDS (Partnered with Peerlogic)
Best for: DSOs and practices standardized on PlanetDDS's Practice Management System (PMS) suite who want to add an AI patient communication layer.
PlanetDDS is a major Practice Management System vendor. While they do not offer a direct AI receptionist, their scale makes them a critical partner ecosystem. AI assistants like Peerlogic integrate deeply with PlanetDDS's platform to serve their large customer base, leveraging real-time booking and two-way data syncs.
4. Scheduling Institute (Partnered with Peerlogic)
Best for: Practices and DSOs that want to combine a strategic training program with an AI assistant to enforce staff accountability and production growth.
The Scheduling Institute is a consulting and training organization focused on operational clarity and scheduling as a growth lever. Their partnership with Peerlogic allows practices to combine their high-touch training and "Enforcement Plan" with Peerlogic's AI platform for 24/7 execution and real-time performance measurement.
5. Resonate AI / DentalBase
Best for: Practices early in the AI evaluation cycle that want a lightweight pilot.
Both Resonate and DentalBase publish strong industry data on the missed-call problem (see DentalBase's data report) and offer entry-level AI call handling. Functional starting points; less mature on enterprise/DSO features.
6. Patient Prism
Best for: Practices that want deep retrospective call analytics and human coaching layered on top.
Patient Prism is primarily an analytics + human-review service for new-patient calls. It is complementary to — not a replacement for — an AI receptionist. Their 2026 call metrics study is one of the most-cited sources in the category.
7. Generic Answering Services (with AI)
Best for: After-hours fallback only.
Traditional answering services charge $1.50–$3.00 per call and have historically taken messages rather than booking appointments. Several have bolted on AI features, but they remain message-takers at heart, with no real PMS integration or call analytics. Use as a fallback layer behind a real AI receptionist, not a primary solution.
How these stack up against the six-point rubric
Across the six evaluation criteria, the practical takeaway is this: most options handle one or two dimensions well, but only a platform approach handles all six. Peerlogic is the only entry above that ships voice AI, texting, engagement, and conversational analytics in a single integrated system — which is why it shows up consistently in Peerlogic case studies with revenue lifts that pure phone tools can't deliver.
Industry context reinforces this. Group Dentistry Now and Becker's Dental Review have both documented the shift from "answering service plus IVR" to integrated AI communication stacks, especially among DSOs scaling past 10 locations. The economics now favor consolidation — practices replacing 2–3 vendors with one AI platform routinely cut tech spend while increasing production.
Practical buying tips
For practices ready to move, three tips that consistently separate good deployments from frustrating ones:
- Start with a baseline. Pull last month's call data — missed rate, after-hours volume, conversion rate. If you can't see this today, that's the first finding. The Peerlogic ROI Calculator gives you a defensible recovered-revenue number in minutes.
- Insist on real PMS integration. "Integrates with Open Dental" should mean two-way real-time booking, not a CSV export. This is the single biggest differentiator between toys and tools.
- Pilot in one location, measure for 30 days, then scale. For DSOs, run the pilot in a middle-performing location, not your best or worst. The 30-day delta will tell you everything.
To see how your specific practice metrics compare, you can use the Dental Practice ROI Calculator to quantify your potential growth.
What is an AI assistant for dental patient calls?
An AI assistant for dental patient calls is a software system that answers, qualifies, and books incoming patient calls automatically, using natural-language conversational AI integrated with your practice management system. Leading options like Peerlogic's Aimee also handle SMS, web chat, and after-hours volume.
How much revenue do dental practices recover with AI call assistants?
Practices using Peerlogic recover an average of $47,000 per year from missed-call follow-up alone, with DSOs identifying $1M+ in annual recoverable revenue across multi-location footprints. Independent industry data from Patient Prism values the average missed call at $200–$300 in immediate revenue.
Are AI dental phone assistants HIPAA-compliant?
The leading dental-specific platforms — including Peerlogic — are built HIPAA-compliant, with BAAs available. Generic VoIP and answering services often require manual configuration to meet HIPAA, so verify before deployment.
Can an AI assistant book into Open Dental, Dentrix, or Eaglesoft?
Yes — but only the dental-specific platforms do this reliably. Peerlogic supports real-time two-way booking with all major dental PMS systems.
Should small practices use AI for phone calls, or only DSOs?
Both. Solo practices typically see the fastest payback because every recovered call lands directly on the schedule. DSOs see the largest absolute dollar impact because the AI catches variance across locations.
What is the "First Mile" of communication?
This refers to the initial contact a patient makes with your practice. When AI agents own this first mile, resolution rates can exceed 75%.
Peerlogic analyzed call data across thousands of dental practices and found that the average practice misses more than $47,000 in annual revenue from calls that go unanswered. This loss occurs before a patient even makes it onto the schedule. Once they are booked, the challenge shifts to retention. Industry research indicates that 15% to 20% of all scheduled dental appointments end in a no-show or same-day cancellation.
When you combine these two figures, a clear picture of the modern dental practice emerges. Offices are losing prospective patients at the first point of contact and then losing booked revenue to schedule gaps. Dental appointment scheduling AI is designed to close both of these leaks by ensuring every call is answered and every commitment is reinforced. According to a 2024 dental industry report, 45% of calls to dental practices occur outside 9-to-5 business hours, meaning nearly half of patient contact attempts happen when most offices are unstaffed.
The average dental practice misses more than $47,000 in annual revenue from calls that go unanswered—a loss that occurs before a patient even makes it onto the schedule.
The Scope of the Dental No-Show Problem
Every practice owner knows the frustration of a fully booked morning that dissolves into empty chairs by noon. While many offices manage this reactively with paper logs or manual follow-up calls, the financial impact of no-shows is often underestimated.
According to a study published by the National Library of Medicine, high no-show rates directly correlate with decreased clinic efficiency and reduced quality of care. For a practice seeing 15 patients per day, a 20% no-show rate means three empty slots. If each slot represents $300 to $500 in production, the annual loss quickly reaches six figures.
Communication breakdowns are the primary driver of this behavior. Patients who cannot reach an office on the first try or who receive inconsistent reminders feel less or no commitment to their appointment time. AI scheduling addresses these friction points by maintaining a constant, reliable line of communication.
How Dental Scheduling AI Operates
Modern AI for dental offices does more than just record messages. It functions as a conversational layer that sits on top of your existing phone lines to resolve patient needs in real time.
Automated Booking and Rescheduling
The AI interprets natural language. If a patient says they have a cracked tooth and need to come in immediately, the system recognizes the urgency, accesses your live integrations with Practice Management Software (PMS), and offers specific available times. The patient receives a text confirmation before the call ends.
Intelligent Missed Call Recovery
If a call comes in while the front desk is occupied or after regular business hours, the system sends an immediate text back. This prevents the "callback lag" that often leads patients to call the next dentist on their search list. Internal data from Peerlogic shows that when patients are prompted by text first, response rates jump to over 60%.
85% of callers who reach a voicemail will not leave a message or call back; they simply move to a competitor who answers.
Information Triage and Knowledge Base
Patients often call for routine details such as insurance accepted, office hours, or post-care instructions. The AI draws from a custom knowledge base to answer these questions at any time of day, allowing your front office team to focus on more complex patient interactions.
Why Missed Calls Are a Greater Revenue Leak Than No-Shows
While no-shows are visible on the schedule, missed calls are invisible losses. The average dental practice fails to answer roughly 30% of its inbound calls. Statistics show that 85% of those callers will not leave a voicemail or call back; they simply move to a competitor.
The Peerlogic dental practice ROI calculator demonstrates that these "ghost" patients represent a significant portion of lost annual production. An AI receptionist solves this by answering every call in under two seconds. One practice implementing this technology reduced their missed call rate from 25% to under 2%, leading to a measurable spike in new patient acquisitions within 60 days.
AI Scheduling vs. Traditional Answering Services
Many practices rely on answering services as a stopgap, but these often create a disjointed patient experience. A traditional service takes a message and promises a callback, which ignores the patient's desire for immediate resolution.
By contrast, AI scheduling provides instant gratification. According to research from Group Dentistry Now, dental groups using AI agents see a 15% to 25% increase in booking conversions over traditional models. Patients prefer finishing the task of booking an appointment rather than waiting for a return call that might come at an inconvenient time.
Practices utilizing AI-driven reminder cadences report a 34% reduction in no-shows compared to those using manual notification systems.
Reducing No-Shows Through Consistent Communication
Bridging the gap between a booked appointment and a completed visit requires three strategic steps:
- Immediate Confirmation: Instant digital receipts for the appointment time.
- Omnichannel Reminders: Sending reminders via the patient's preferred method (text or email).
- Self-Service Rescheduling: Allowing patients to move appointments without needing to call the office.
Implementation Strategies for Success
To get the most out of conversational insights, consider the following steps:
- Synchronize Your Calendar: Ensure your AI is fully integrated with your PMS for real-time availability.
- Audit Your Call Flows: Identify the times of day when your team is most overwhelmed to deploy AI support.
- Review Summaries Daily: Use AI-generated call summaries to keep the clinical team informed on patient needs.
AI handles the volume; your team handles the nuance. This combination typically produces a 50% reduction in front office workload.
Does AI scheduling work with my current dental software?
Yes, Peerlogic integrates with major platforms like Dentrix and Dentrix Ascend to provide a seamless scheduling experience.
Can patients tell they are talking to an AI?
Modern AI uses natural language processing to provide a human-like, helpful experience that focuses on resolving the patient's request quickly.
What happens if the AI can't answer a question?
The system is designed to triage complex queries and hand them off to your front office team with a full transcript of the interaction so no context is lost.
Conclusion
The shift toward AI in dental practice management is centered on one goal: increasing production through better communication. By answering every call and reinforcing every appointment, practices can stop reactive management and start scaling effectively.
If you are ready to see how Aimee, Peerlogic’s AI assistant, can support your front desk and fill your chairs, book a demo today.
A patient calls your office at 7:15 PM on a Tuesday. They are experiencing sharp pain and are ready to book an emergency appointment. In most offices, this call goes to a voicemail that 87% of patients will never leave a message on, according to internal Peerlogic research. To solve this, many practices are turning to automated answering services. The promise is enticing: 24/7 availability, no hold times, and a virtual dental receptionist that never takes a lunch break.
However, a significant problem has emerged. While many tools can "answer" a phone, few can actually "manage" the patient. A generic AI often lacks the clinical nuance to distinguish between a routine cleaning and a high-value periodontal case. This gap is expensive. Recent industry data suggests that dental practices miss roughly 35% of their 40–60 daily calls, leading to a loss of $2,800–$6,300 in immediate revenue every single day.
If your AI tool is simply checking boxes instead of understanding intent, you aren't solving the problem—you are just automating the loss of revenue.
The Difference Between Answering and Understanding
Most dental practices evaluate a virtual receptionist based on uptime: Did it pick up the phone? While uptime matters, it is the wrong metric for growth. The question that dictates your ROI is whether the AI understands what the patient is asking for and how to convert that inquiry into a booked chair.
Consider these common scenarios where basic AI fails:
- Clinical Nuance: Failing to prioritize an emergency patient over a billing question.
- Insurance Verification: Providing vague answers about coverage that cause the patient to "shop around" elsewhere.
- Tone and Empathy: Sounding like a robotic script rather than a professional extension of your local practice.
Why Specialized Dental AI Wins
The market is currently flooded with general-purpose AI tools that have been given a "dental skin." These tools usually fall short because they lack conversation intelligence. Without this layer of technology, your practice remains blind to why patients are hanging up or why certain procedures aren't being booked.
According to a 2024 ADA Health Policy Institute survey, 62% of dentists cited staffing shortages as their primary challenge. When your front office is stretched thin, you cannot afford an AI tool that requires constant "babysitting" or manual data entry.
Four Critical Features of True Conversation Intelligence:
- Deep Integration: The AI must talk directly to your practice management software (PMS) to see real-time availability.
- Intent Mapping: Identifying if a caller is a "new patient" versus an "existing patient" to apply the correct script and priority.
- Automatic Follow-Up: If a high-value call drops, the system should immediately trigger a text back to save the lead.
- Sentiment Analysis: Monitoring the caller’s frustration or urgency to alert the human team when a personal touch is needed.
Turning Missed Opportunities into Production
The real problem with basic AI receptionists isn't that they answer calls poorly—it's that they answer them blindly. They provide a "wall" for the caller to hit rather than a bridge to the practice.
Data shows that 45% of calls to dental practices occur outside of traditional 9-to-5 business hours. If your automated solution doesn't have the intelligence to capture those leads effectively, you are losing nearly half of your potential patient growth.
Practices that switch from generic answering services to dental-specific AI like Aimee see a dramatic shift in their bottom line. In fact, AI-driven follow-up has been shown to recover over $47,000 in a single month across a group of practices by capturing the revenue most offices never even knew they were losing.
Does Peerlogic replace my front desk staff?
No. Peerlogic is designed to support your team by handling after-hours calls, lunch breaks, and high-volume periods so your staff can focus on the patients physically in the office.
How long does it take to train the AI?
Unlike general AI, dental-specific platforms are pre-trained on millions of dental industry data points, allowing them to be operational almost immediately after integration with your PMS.
Can the AI handle emergency calls differently?
Yes. Advanced conversation intelligence identifies keywords related to pain or emergencies and can route those calls or alerts with higher priority than routine inquiries.

The operational gap behind missed calls and lost revenue
For Gen4 Dental Partners, a DSO overseeing 100+ practices, growth efforts often focus on paid media and SEO.
However, as VP of Marketing Amy McNeill discovered, the patient experience at the front desk determines whether that demand turns into booked appointments.
By implementing Peerlogic, Gen4 gained full-funnel visibility into what was actually happening when the phone rang—revealing that when inbound calls go unanswered, revenue leaves immediately.
At scale, the gap becomes harder to see without centralized visibility. As organizations add locations through growth and M&A, they often inherit different systems, people, and processes that are not congruent across the portfolio.
Without a centralized way to understand what is happening in patient conversations, it becomes difficult to enact change, support offices, or measure performance consistently.
Centralizing phone systems to create visibility and accountability
A practical starting point is centralizing phone systems to create a single source of truth. In a single-scaled environment, operations were spread across roughly 15 phone systems, and only one provided usable data. Centralization made it feasible to understand performance across locations and begin improving offices with consistent reporting.
Change management remained a core consideration. The shift was not only a technology change but also a people-and-process change. A phased rollout reduced friction: onboarding took about six months, with 10–15 offices launched per month.
The initial focus was simply to replace phone systems and allow data to populate, without introducing a large training program at the start. This approach helped avoid overwhelming staff and created space to learn from the data before implementing targeted training.
Early metrics that reveal the gap: missed call percentage
Missed call percentage emerged as an early metric because it required minimal training and created immediate clarity. Simply making the metric visible and known across offices produced an organic improvement: missed call percentage dropped by about 2% after teams learned that centralized reporting existed.
At the portfolio level, small percentage changes translated into large volumes. When missed calls were analyzed more granularly for new patient calls, the impact was quantified at roughly 700 new patients per month. Performance also varied widely by location, with some offices near 5% missed calls and others near 50%. This variability highlighted where marketing spend was undermined by operational breakdowns, including instances in which leads costing $250 or more went directly to voicemail.
Understanding the modern patient journey and why conversion breaks down
New patient behavior reflected a strong preference for immediacy. Patients often complete research before calling, including reviewing websites and reading reviews, and then call with the intent to book quickly. When voicemail is reached, the next call often goes to another practice. Waiting for a callback or waiting months for an appointment creates friction that prevents booking.
Conversion issues were not limited to answering the phone. Once call data became available, it was possible to separate new- and existing-patient performance and identify reasons for not being booked. One major driver was scheduling access. Data showed that 38% of new patients who did not convert were lost due to scheduling constraints, prompting broader operational work on scheduling and a goal of getting new patients in within 7 days. This also surfaced the importance of tracking availability metrics such as the "3rd next available appointment."
Reasons not booked: insurance handling, scheduling, and cancellations
Call listening and categorization revealed recurring breakdowns that created missed booking opportunities. Insurance was a major factor. In one common scenario, a patient mentioned an insurance plan such as Delta Dental and received an immediate "we don't take that," ending the call without exploring whether insurance was the deciding factor or whether alternatives existed. This was especially costly when acquisition costs were high and the call ended prematurely.
Cancellations were another area where training and process mattered. Calls to cancel were sometimes handled with minimal resistance, rather than reinforcing the value of the reserved time and encouraging the patient to keep the appointment when possible. These were treated as high-impact categories because shifting just one or two priority behaviors by 1–2 percentage points could translate into hundreds of thousands of dollars per month across a large footprint.
Measuring revenue impact with simple benchmark math
Revenue impact was modeled using benchmark inputs observed across a broad portfolio. Using a simplified per-location example:
- 100 inbound calls per week
- 38% missed call rate (≈ 38 missed calls/week)
- ~40% blended conversion rate on those missed calls (≈ 15 lost bookings/week)
- $300 average appointment value
Under these assumptions, a single location is leaving roughly $4,500 per week — about $19,500 per month — on the table.
At portfolio scale, the math compounds quickly. Across a multi-location footprint, mid-sized DSOs commonly model six-figure monthly recovery opportunities, and larger groups frequently surface $450,000+ per month in unbooked revenue. The underlying point is consistent: benchmarking performance, measuring missed opportunities, and tracking improvements creates a measurable mechanism for top-line acquisition and operational optimization.
Deploying AI without overcomplicating workflows
AI adoption tended to fall between two extremes: avoiding it due to concerns about patient acceptance, or expecting it to solve everything immediately. A phased approach aligned better with operational reality. AI was positioned as a support layer rather than a replacement for front desk teams, addressing common fears such as job loss or increased workload.
Practical AI use cases focused on reducing missed opportunities and improving responsiveness:
- Handling missed calls through AI voice or rapid missed-call-to-text follow-up
- Supporting after-hours and weekend inquiries, when staff are not working
- Enabling online scheduling across locations
- Automating appointment reminders and messaging to fill schedules after cancellations
- Using AI in reporting and analysis workflows
- Applying AI in clinical contexts such as scans in the chair
This approach emphasized "human first" when teams were trained and available, while using AI to prevent calls from going to voicemail, reduce hold times, and allow staff to focus on in-office patient interactions, empathy, and emergencies.
Implementation implications: training, peer adoption, and iteration
AI performance depended on training and configuration. Incorrect responses—such as directing emergency patients elsewhere—were treated as issues to resolve by training the agent to respond as intended, including using specific words and phrasing to guide behavior.
Adoption also benefited from peer-to-peer reinforcement. Some offices felt compelled to jump into AI-driven conversations, creating disjointed experiences and additional workload through parallel message threads. Other offices allowed workflows to run and saw time savings. Bringing peers together to share how they used the tools helped reduce apprehension and generated feedback to optimize responses, booking behavior, and workflows.
Key implications for scalable growth
Centralized phone data laid the foundation for measurable improvement by establishing benchmarks, accountability, and visibility into front-desk operations. Early wins came from focusing on simple metrics like missed call percentage, then expanding into deeper insights such as reasons not booked, insurance objections, cancellations, and scheduling access.
Small improvements in core metrics produced an outsized financial impact across multi-location environments. The operational path emphasized prioritization over complexity: identify the highest-percentage reasons for lost bookings, address them with targeted training and workflow changes, and iterate using measurable reporting.
AI fit into this model as a support layer that improves responsiveness and reduces friction, particularly during high-volume periods, lunch, after-hours, and weekends.
Take the Next Step: Audit Your Practice Performance
The success seen at Gen4 Dental Partners demonstrates that visibility is the first step toward significant revenue recovery. To see how many opportunities your own practice might be missing, you can access a detailed analysis and the full webinar insights today.
Access the 14-Day Practice Call Audit & Full Webinar Replay here.
38% of DSO revenue flows directly through the phone — new patient acquisition, case acceptance, hygiene utilization, reactivation. Every dollar of growth you're planning begins with a conversation. That means scaling from three locations to five doesn't just multiply your capacity. It multiplies every communication gap that already exists across your current offices. The practices that expand without fixing their phone infrastructure first don't just struggle — they lose revenue in ways that never show up in a production report.
The Numbers That Define What Expansion Actually Costs You
Before your fourth or fifth location opens its doors, consider what is happening right now across your existing three:
- 25–40% of new patient calls to dental offices do not result in a booked appointment — even when someone picks up the phone. (Peerlogic)
- Dental practices miss an average of 28–38% of incoming calls during normal business hours, with some locations running miss rates as high as 68%. (Resonateapp.com)
- Only 14% of new patients leave a voicemail when their call goes unanswered. The other 86% call the next practice on their list. (DenteMax)
- 58% of all missed call interactions involve new patients — the highest-value callers your marketing budget is paying to attract. (TrueLark, 8 Million Patient Conversations)
- Each missed new patient call represents approximately $850 in immediate first-year revenue and up to $8,000 in lifetime patient value. (Resonateapp.com)
- For dental groups, 38% of total revenue flows through the phone — new patient acquisition, case acceptance, hygiene utilization, and reactivation all begin with a conversation. (Peerlogic)
At three locations, that revenue leak is painful but manageable. At five, it is structural — and invisible, because the money never appeared in the first place. You cannot see it in a production report. You cannot find it in a reconciliation. It simply does not exist.
According to Peerlogic's 2026 State of Dental Best Practices research, only 36% of practices review communication performance data weekly. The majority are expanding on assumptions. For a dental group owner moving from three to five locations, that is the most expensive operational blind spot in your business.
Why 3 Locations Is the Real Inflection Point
Most dental group owners who are running two or three locations successfully have gotten there through a combination of clinical reputation, good local marketing, and an operations model built on personal involvement. The owner knows the front desk teams by name. The owner has a feel for which location is converting well. The owner can walk into any of the three offices on any given morning and get a read on how things are going.
At four and five locations, that model breaks — not because the owner stops caring, but because it physically cannot scale.
Open Dental's multi-location scaling research names the risk directly: "The infrastructure decisions you make at 5 locations determine what's possible at 50." The systems you have at three locations — your communication workflows, your training processes, your reporting structure, your technology stack — were designed to work with the owner in the building. They were not designed to work without them.
Curve Dental's practice growth analysis documents the same shift: the founding dentist must move away from direct operational management and toward systems, data, and centralized visibility at the three-to-five location stage. Practices that make that transition cleanly scale well. Practices that try to replicate a personal oversight model across five locations produce inconsistent patient experiences, widening performance gaps between locations, and an owner who is stretched thin across everything and effective at nothing.
Patient communication is almost always the first system to break — and it breaks in ways that are quiet, invisible, and expensive.
The Three Ways Patient Communication Breaks When You Scale
1. Call Volume Outpaces Front Desk Capacity — and You Can't See It
At one well-staffed location, inbound call volume is manageable. Add a second and third location, and each team is managing its own call volume independently — with no overflow capability between offices and no shared visibility into how each location is actually performing on the phone.
Peerlogic's research identifies 3:00 PM as the peak call volume window — exactly when front desk teams are managing patient check-outs, running end-of-day reconciliation, and fielding the afternoon wave of appointment confirmation calls. Without AI-assisted call handling, that 3:00 PM window is where new patient calls go unanswered at the highest rate, every single day, across every location.
Multiply that across five locations on five separate phone systems and you have a predictable, daily revenue drain that no amount of hiring solves cost-effectively. The average dental practice misses approximately 40 new patient calls per month. At five locations, that is 200 missed new patient opportunities per month — before you have even opened your door on a single new acquisition day.
2. Performance Variability Becomes Invisible and Unmanageable
At one location, you know which front desk team member converts well on the phone and which one loses patients on insurance questions. You have heard the calls. You have coached the team. You have a direct line of sight to where the gaps are.
At five locations, you have no idea.
You are relying on location managers to surface problems — which means you only hear about failures visible enough to escalate. The invisible failures — new patient calls converted at 38% instead of 58%, insurance objections that went unanswered, after-hours calls that got answered but never booked — never reach your desk. They just quietly do not show up as revenue.
McKinsey projects the U.S. dental industry will be short more than 36,000 dental professionals by 2031, and a 2024 DentalPost Salary Report found that over 50% of dental professionals are actively or passively seeking new positions. The front desk team you hire at location four today has maybe a 50/50 chance of still being there in 18 months. Without a system that trains, monitors, and coaches that person automatically — from day one and continuously — you are betting your new patient conversion rate on whoever shows up and however well your location manager remembered to train them.
3. Your Revenue Cycle Has No Consistent Starting Point
At a single location, your front desk team develops phone habits over time — some good, some not. At five locations, five different teams develop five different sets of habits. Some handle insurance questions well. Others don't. Some create urgency with new patients calling about pain. Others treat every call like a scheduling transaction.
The result: your revenue cycle starts from a different place at every location, depending on which team member answered the phone, what mood the patient caught them in, and whether the location manager happened to run a training session recently.
Dental practice overhead averages 60–65% of production and is rising, meaning every dollar of production your phone conversations fail to capture has an outsized impact on your margins. For a five-location group producing $200,000 per location per month, even a 5% improvement in new patient call conversion represents $50,000 in additional monthly production — without adding a single provider, a single marketing dollar, or a single new service.
What You Need to Fix Before Location Four Opens
Centralized Call Intelligence — Not Just Coverage
The most common mistake dental group owners make at this stage is solving the coverage problem — making sure calls get answered — without solving the intelligence problem — understanding what is happening in those calls and whether they are converting.
Tools that answer the phone are valuable. A virtual dental receptionist that operates 24/7 and captures after-hours calls is meaningfully better than voicemail. But if that tool cannot tell you your new patient call conversion rate by location, by time of day, and by team member — and cannot surface the specific conversations where patients disengaged and why — you are managing the channel blind.
As Peerlogic CEO Ryan Miller has noted: "If 2025 was a year of recalibration, 2026 is a year of intention." For dental group owners scaling from three to five locations, intention means replacing assumption-based management with data-driven visibility — starting with the phone.
A Coaching Loop That Does Not Depend on You Being There
The traditional model for front desk coaching is: manager listens to calls occasionally, identifies a problem, runs a training session, and hopes it sticks. At one location, that model is imperfect but functional. At five locations, it is not functional at all.
What you need is a platform that automates the coaching loop — flagging specific calls where a conversion opportunity was missed, identifying the exact moment in the conversation where the patient disengaged, and delivering that feedback to the team member and location manager without requiring a manual review process.
Fortune Management's dental scaling research identifies systematic, consistent training as the backbone of scalable growth — but notes that "technology alone won't solve all your problems" if the team is not being developed alongside it. The right dental AI assistant does both: it handles the calls that the team cannot handle, and it makes the team better at the calls that require a human.
PMS Integration That Works Across All Your Locations
Before your fourth location opens, every system in your patient communication stack should be fully integrated with your practice management software — not surface-level connected, but deeply integrated, reading appointment types and provider schedules and writing confirmed bookings and call outcomes back into the system automatically.
Curve Dental's scaling research notes that one of the most common mistakes early-stage dental groups make is continuing to operate multiple disconnected practice management systems after acquisitions — a fragmentation that compounds quickly once AI tools are layered on top. Open Dental's enterprise scaling guide puts it plainly: "Fragmented systems produce fragmented insights." If your communication platform does not connect seamlessly to your PMS, every location you add widens that fragmentation rather than resolving it.
Benchmarking Before You Need It
Most dental group owners at three locations do not have performance benchmarks — conversion rate targets by location, new patient call answer rate minimums, after-hours booking percentage goals. They operate by feel and by comparison to last month.
At five locations, benchmarks are not optional. They are the mechanism by which you identify underperformance before it becomes a crisis, recognize strong performers before they leave for a competitor, and make technology and staffing decisions based on data rather than gut.
DentalBase ROI research finds that practices implementing AI-assisted call intelligence recover 60–80% of previously missed patient opportunities — but only when the system is configured against clear performance targets, not simply deployed and forgotten. Benchmarks are the difference between deploying a tool and running a system.
8 Questions to Ask Yourself Before Opening Location Four
These are the operational readiness questions that separate dental group owners who scale cleanly from those who find themselves at five locations wondering why their new patient numbers are not where they expected.
Question 1: Can I see my new patient call conversion rate at each of my three current locations right now?
Not call volume — conversion rate. New patient calls received divided by new patient appointments scheduled, broken down by location. If the answer is no, you are expanding without knowing whether your most important revenue channel is working. Fix this before you sign a lease.
Question 2: Do I know which front desk team member at each location is my strongest phone converter — and which is costing me patients?
If you cannot answer this by name, you do not have visibility into your front desk performance. A conversation intelligence platform surfaces this automatically, without requiring you to listen to calls or rely on manager reports.
Question 3: What happens to a new patient call that comes in at 7:45 PM at any of my three locations?
If the answer is voicemail, you are losing at least 86% of those callers to competitors. An AI dental receptionist that answers after-hours calls and books appointments in real time is not a luxury at five locations — it is a baseline requirement for not leaving money on the table every evening.
Question 4: How long does it take to onboard a new front desk hire to your phone performance standards?
If the answer is "a few weeks with the manager" or "we train them on the PMS and hope for the best," your training process does not scale. A new hire at location four who receives automated, call-level coaching from day one will reach conversion performance benchmarks faster and more consistently than one who learns by shadowing a colleague who may or may not have strong habits themselves.
Question 5: Do my five front desk teams use the same language to describe treatment urgency, insurance options, and pricing?
Inconsistency in how treatment is presented over the phone directly affects case acceptance rates. Research across dental practices shows that the way a front desk team describes a procedure — its urgency, value, and process — directly affects whether a patient accepts it. If five teams are using five different scripts, you have five different case acceptance rates — and no way to know which is best.
Question 6: What is your plan for managing call overflow when two locations have peak call volume at the same time?
Without centralized call handling infrastructure, peak periods at multiple locations simultaneously create compounding miss rates. AI call answering for dental clinics that routes overflow intelligently and handles after-hours volume at all locations from a single platform eliminates this problem structurally rather than patching it with more hires.
Question 7: Can my current technology stack produce a single report showing production, call conversion, and new patient trends across all three locations this week?
If producing that report requires exporting from three different systems, emailing three location managers, and building a spreadsheet on Sunday evening — you do not have a management infrastructure for five locations. You have three separate single-location businesses held together by your personal attention. That does not scale.
Question 8: Does your AI or call tool vendor have documented experience with group practices at your stage of growth — and can they give you a reference?
A vendor who has successfully deployed across 3–10 location dental groups has worked through the PMS integration challenges, the multi-location coaching workflows, and the enterprise reporting requirements you will encounter. A vendor who has only served single-location practices is learning on your time. Ask for two current group practice clients at a similar scale. The call will take 20 minutes and tell you more than any demo.
What Solving This Looks Like Before Location Four Opens
The practices that scale from three to five locations cleanly — without losing new patient volume, without front desk chaos at the new location, without the owner becoming the emergency fix for every communication breakdown — have one thing in common: they built their communication infrastructure before they needed it at that scale.
That means:
- A dental AI assistant platform deployed across all current locations, producing consistent conversion data and coaching insights, before the fourth location inherits the same gaps the first three have been quietly carrying
- PMS integration that is fully operational and tested across all existing locations, so the new location onboards into a working system rather than a fragmented one
- Benchmarks established from current location data, so you know what "good" looks like before you try to hold a new team accountable to it
- A coaching workflow that runs automatically, without requiring the owner or a dedicated QA manager to listen to calls manually
One dental practice that combined Peerlogic's conversation intelligence platform with Scheduling Institute's 5-Star Telephone Training booked 244 additional appointments, generating over $204,000 in additional annual revenue — not from marketing spend, not from a new location, but from converting more of the new patient calls they were already receiving.
At five locations, that math multiplies. So does the cost of not solving it.
Frequently Asked Questions for Growing Dental Group Owners
When should a dental group start investing in AI call intelligence — at 1 location or 3?The earlier the better, but the inflection point where it becomes strategically critical is the 3–5 location window. That is when personal oversight stops scaling and when performance data across locations becomes the only reliable management tool.
How does conversation intelligence differ from just adding an AI receptionist?An AI receptionist answers calls and books appointments. A conversation intelligence platform analyzes what happens in every call, surfaces missed conversion opportunities, coaches front desk teams automatically, and connects call outcomes to production revenue. The first solves a coverage problem. The second solves a revenue optimization problem.
What is a realistic new patient call conversion benchmark for a well-run dental group?Top-performing practices convert 55–75% of answered new patient calls to appointments. Industry average is approximately 42%. A multi-location group with no centralized call intelligence or coaching infrastructure typically runs below average at several locations without knowing it.
How long does it take to implement Peerlogic across multiple locations?Peerlogic integrates with major PMS systems including Dentrix, Eaglesoft, and Open Dental, and is designed for multi-location deployment without requiring rework at each new location. Contact Peerlogic directly for a deployment timeline based on your specific setup.
What is the biggest mistake dental group owners make at the 3–5 location stage?Assuming that what worked operationally at two locations will work at five. The most common specific failure is not having centralized visibility into phone performance — which means revenue gaps exist across all locations simultaneously, compounding, without ever appearing on a report.
→ See how Peerlogic helps dental groups scale patient communication without losing control.→ Request a practice analysis to find where your current locations are leaving revenue on the table.→ See how Peerlogic's conversation intelligence platform works for practices of all sizes.
Sources: Peerlogic – Scale Without Losing Control | Peerlogic / Scheduling Institute | Resonateapp.com | TrueLark 8M Conversations | DenteMax | New Patients Flow | Open Dental Scaling Guide | Curve Dental Multi-Location Growth | DentalBase ROI Guide | DentalPost 2024 Salary Report via AADOM | McKinsey Dental Staffing via Pearly | Fortune Management Scaling | Dental Practice Insider Growth Guide | Dental Office Production Benchmarks 2026 | PracticeCFO Dentistry 2026
Front office staff spend nearly 40% of their day on repetitive administrative tasks — almost half their bandwidth gone before they speak to a single patient. That's the gap AI receptionist tools are trying to close. But not every tool is solving the same problem, and the differences between platforms matter far more than most comparisons will tell you. Here's an honest look at what Arini does, where it falls short, and how it stacks up against a platform built specifically for dental revenue intelligence.
The Stat That Should Frame Every AI Receptionist Decision
Before comparing any two tools, it helps to understand what you are actually trying to solve.
- 25–40% of new patient calls to dental offices do not result in a booked appointment — even when the call is answered. (Peerlogic)
- Dental practices miss 28–38% of incoming calls during business hours. (Resonateapp.com)
- Only 14% of new patients leave a voicemail when their call goes unanswered. The rest call a competitor. (DenteMax)
- 58% of all missed call interactions involve new patients — your most valuable callers. (TrueLark)
- Each missed new patient call represents approximately $850 in immediate revenue and up to $8,000 in lifetime patient value. (Resonateapp.com)
These numbers define two distinct problems: the coverage problem (calls going unanswered) and the conversion problem (answered calls not booking). Tools like Arini are built primarily to solve the coverage problem. Platforms like Peerlogic are built to solve both — and to add a third layer: the intelligence problem, which is understanding why conversion succeeds or fails in the first place.
That distinction is the entire basis for this comparison.
What Is Arini?
Arini is an AI receptionist built specifically for dental practices. It was founded by Abdul Alim and Rami Odeh — both former engineers at Threads, an enterprise communication platform — who identified the dental front desk as a significant and underserved bottleneck after going door-to-door to dental offices and shadowing practice staff. (Y Combinator)
The core product is a voice-based AI that answers inbound phone calls, handles patient questions, and books appointments directly into the practice's scheduling system. Arini markets itself as a 24/7 AI dental receptionist — available when human staff are not, capable of handling high call volumes without hold times, and integrated with a wide range of practice management software.
According to Arini's Y Combinator listing, the dental front desk spends approximately 6 hours per day on the phone — and still misses 35% of calls. Arini's value proposition is straightforward: answer 100% of calls, reduce the administrative burden on front desk staff, and capture new patient opportunities that would otherwise go to voicemail or to competitors.
What Arini Does Well
Based on publicly available information, user reviews, and third-party comparisons, Arini's strengths include:
Natural-sounding voice interaction. Arini is consistently noted for voice quality and conversational naturalness. Review aggregators and dental-specific evaluations describe patient experiences as comparable to speaking with a human receptionist — which is critical for a front-office application where patient comfort and trust are foundational.
Dental-specific training. Unlike repurposed general-purpose AI tools, Arini was built from the ground up for dentistry. It understands dental terminology, procedure types, common patient concerns, and scheduling contexts. This shows up most clearly in its ability to handle questions about specific procedures and to recognize when a patient may need to be triaged as an emergency.
Broad PMS and phone system compatibility. Arini integrates with Open Dental, Eaglesoft, Denticon, and other major practice management systems, as well as a wide range of dental phone providers including Weave, Mango, and GoTo. For practices that are hesitant to change their existing infrastructure, this compatibility reduces friction significantly.
24/7 availability. This is the core use case Arini was built around. Practices that were previously routing after-hours calls to voicemail — and losing the 86% of new patients who will not leave a message — gain immediate value from a system that picks up at 10 PM and books the appointment in real time.
HIPAA compliance. Arini maintains HIPAA compliance with strong encryption protocols and continuous compliance monitoring via SecureFrame. For practices concerned about patient data handling, Arini can produce documentation of its compliance posture.
Multilingual support. Arini handles patient conversations across multiple languages, which is particularly valuable for practices serving diverse patient demographics in markets with significant non-English-speaking populations.
For smaller practices or single-location offices looking for a virtual dental receptionist that solves the coverage problem cleanly — without heavy configuration or extensive onboarding — Arini is a legitimate and well-reviewed option.
Where Arini Has Limitations
Understanding Arini's limitations requires understanding what the product was designed to do and what it was not.
Arini is a call-answering and scheduling product. Its primary focus is coverage: making sure the phone gets answered, questions get addressed, and appointments get booked. That is a meaningful and genuinely valuable function.
What Arini's core product does not provide in the same depth as a full conversation intelligence platform:
Conversion analytics. Arini offers an analytics dashboard that shows call metrics and booking performance. What it does not provide is the deep conversion intelligence a platform like Peerlogic delivers — the ability to see, for every call, exactly where the patient disengaged, which objection went unanswered, which team member missed the conversion opportunity, and how that individual call maps to your revenue cycle.
Coaching recommendations. Arini's value is in automating call handling. It does not provide a structured coaching loop that automatically surfaces missed conversion moments to front desk managers or team members and tracks performance improvement over time. For practices serious about developing their human team's phone skills alongside AI automation, that gap is significant.
Revenue cycle connection. Arini can tell you that a call resulted in a booking. It is not designed to connect that call to treatment acceptance rates, production data, or patient lifetime value in the way a purpose-built conversation intelligence platform can.
Enterprise-grade multi-location reporting. Third-party comparisons note that Arini has focused on the DSO market and supports multi-location deployments, but enterprise-level cross-location performance benchmarking — the ability to compare conversion rates across 20 locations, rank them, and drill into the specific call patterns explaining the variance — is where platforms purpose-built for DSO intelligence pull ahead.
These are not criticisms of Arini as a product. They are honest observations about what the product was built to do and where the architecture of a call-answering tool hits its natural ceiling.
Arini vs. Peerlogic: Two Different Categories of Tool
The most important thing to understand about this comparison is that Arini and Peerlogic are not direct competitors fighting for the same buyer with the same needs. They occupy adjacent but distinct categories in the dental AI landscape — and confusing them leads to mismatched purchasing decisions.
Arini is a virtual receptionist. Its primary function is call coverage — ensuring that patient calls are answered, questions are addressed, and appointments are booked, 24/7, without requiring additional front desk staff.
Peerlogic is a conversation intelligence platform that includes AI call handling as one component. Its primary function is revenue optimization — surfacing the intelligence from every patient conversation, connecting that intelligence to production data, and using it to improve both AI and human performance over time.
Here is how that difference plays out in practice:
QuestionAriniPeerlogicDoes it answer calls 24/7?YesYesDoes it schedule appointments?YesYesDoes it integrate with major PMS systems?YesYesDoes it report call-to-appointment conversion rates?LimitedYes, with drill-downDoes it surface missed conversion opportunities?Not by designYes, automaticallyDoes it coach front desk teams with specific call feedback?NoYesDoes it connect calls to production revenue data?NoYesDoes it support multi-location enterprise benchmarking?LimitedYes, purpose-builtDoes it identify insurance objection patterns across your team?NoYes
The right choice depends entirely on what problem you are trying to solve.
If your primary pain point is after-hours coverage and call volume overflow — and you want a clean, natural-sounding solution that integrates with your existing PMS without heavy configuration — Arini is a reasonable and capable tool.
If your primary pain point is understanding why your practice is leaving revenue on the table and systematically fixing it — and especially if you are operating at DSO scale where that question multiplies across multiple locations — Peerlogic provides a fundamentally different level of capability.
5 Questions to Ask Before Choosing Between Them
1. What is your primary goal: coverage or conversion intelligence?
If the answer is coverage — answering the phone 24/7 and reducing missed calls — Arini solves that problem. If the answer is conversion intelligence — understanding why calls are not converting and using that data to improve performance — that requires a platform designed around analytics, not just call handling.
2. Do you need to coach your front desk team, or just supplement them?
Arini is designed to handle calls your team cannot handle. Peerlogic is designed to both handle calls and make your team progressively better at the calls that require a human. If staff development and consistent performance are priorities — particularly for practices dealing with turnover or multi-location inconsistency — the coaching layer matters.
3. How many locations are you operating or planning to operate?
For a single location, the differences between Arini and Peerlogic matter less. For a practice scaling to 5, 10, or 20+ locations, the ability to benchmark performance across locations, identify outliers, and systematically coach distributed teams at scale determines whether your AI investment generates compounding returns or plateaus.
4. Can you connect call performance to production data?
For practice owners and DSO operators who manage their business with production metrics — which is the standard in dental — the ability to link phone performance to revenue is the difference between measuring a channel and measuring its output. Peerlogic provides that connection. Arini, as a call handling product, does not.
5. What happens when an AI call does not convert? Can you see why?
This is the diagnostic question. Ask any vendor: show me a call that did not convert to an appointment, and show me what your platform tells me about why. The depth of that answer reveals more about the platform's actual intelligence than any feature checklist.
Who Should Choose Arini
Arini is a well-built, dental-specific virtual receptionist that makes sense for:
- Single-location practices whose primary problem is after-hours call coverage
- Practices looking for a low-friction, fast-to-deploy AI call answering solution without heavy configuration
- Practices that have strong front desk teams and primarily need the AI to handle overflow and after-hours volume
- Operators who want to solve the coverage problem now and add intelligence capabilities later as the practice grows
Who Should Choose Peerlogic
Peerlogic is the right choice for:
- Practices and DSOs that want to understand and optimize the revenue impact of every patient conversation
- Multi-location operators who need cross-location benchmarking, centralized reporting, and systematic coaching at scale
- Practices that have already tried a basic AI call tool and found that new patient numbers are still flat
- Organizations where front desk team performance variability is creating inconsistent conversion rates
- DSOs evaluating AI as a strategic revenue tool, not just an operational convenience
One practice using Peerlogic alongside Scheduling Institute's training booked 244 additional appointments and generated over $204,000 in additional annual revenue — not from more marketing spend, but from converting more of the calls already coming in.
That is the difference between a coverage tool and a revenue intelligence tool.
Frequently Asked Questions
Is Arini good for DSOs?Arini supports multi-location deployments and has features relevant to DSOs, including a centralized dashboard and consistent call handling across locations. For DSOs that primarily need call coverage standardization, it is a viable option. For DSOs that need deep cross-location conversion analytics, automated coaching workflows, and revenue cycle connection, a platform like Peerlogic provides meaningfully more capability.
How does Arini pricing compare to Peerlogic?Arini does not publish pricing publicly and requires a demo call to get specific numbers. Peerlogic similarly provides custom pricing based on practice size and needs. The more important financial comparison is total value: what does each platform contribute to your revenue per dollar spent? A higher-cost platform that generates $200,000 in recovered annual revenue is a better investment than a lower-cost platform that produces no measurable revenue impact.
Can I use both Arini and Peerlogic together?In some configurations, Arini's call answering layer and Peerlogic's conversation intelligence layer could complement each other. However, Peerlogic's platform includes AI call handling as a native component, which may reduce the need for a separate call answering product. Contact Peerlogic directly to discuss your specific setup.
What is the best dental AI receptionist in 2025–2026?The answer depends on what you are optimizing for. For call coverage, Arini is among the better-regarded options in the market. For revenue intelligence, coaching, and enterprise-grade analytics, Peerlogic is the most purpose-built solution available for dental practices and DSOs.
How do I evaluate which AI dental tool is right for my practice?Ask every vendor the same question: after a call ends, what can you tell me about it? The depth of the answer tells you everything about whether you are buying a phone system or a revenue tool.
→ See how Peerlogic's conversation intelligence platform compares to standalone AI receptionist tools.→ Request a demo to see Peerlogic's patient acceptance data in action.→ Request a practice analysis to see where your current setup is leaving revenue on the table.
Sources: Peerlogic / Scheduling Institute | Resonateapp.com | TrueLark 8M Conversations | DenteMax | Arini.ai | Arini Y Combinator | Futurepedia Arini Review | TensorLinks vs. Arini Comparison | mConsent Top AI Receptionists 2026 | DentalBase ROI Guide | Oral Health Group | New Patients Flow | Arini.ai Improve Missed Calls

89% of patients say they would consider switching dental providers after a poor phone experience — including long hold times, difficulty scheduling, or unanswered questions. If your AI receptionist is not turning calls into booked appointments, it is not solving that problem. It may be making it worse.
There are two sets of numbers every dental practice should know. The first is how many calls your practice receives. The second is how many of those calls convert to booked appointments.
Most practices know the first number. Almost none know the second.
Here is why that gap is dangerous:
- 25–40% of new patient calls to dental offices do not result in a scheduled appointment — even when the call is answered. (Peerlogic)
- Only 68% of new patient calls are answered in the first place — and of those, only 42% convert. (Peerlogic / Scheduling Institute)
- Practices miss an average of 28–38% of incoming calls during business hours. (Resonateapp.com)
- 58% of missed call interactions involve new patients — your most valuable callers. (TrueLark)
- Each missed new patient call costs approximately $850 in immediate revenue and up to $8,000 in lifetime value. (Resonateapp.com)
If you adopted a dental AI receptionist specifically to close these gaps — and your practice still cannot answer the question "what is our call-to-appointment conversion rate?" — there is a problem. And it is almost certainly costing you more than you realize.
This guide is for practices that have already tried AI call technology and are not sure whether it is working. We will walk through exactly how to tell if your solution is failing, why it is failing, and what the path forward looks like.
Warning Sign #1: You Have No Visibility Into Call Outcomes
This is the single most common — and most costly — failure mode in dental AI receptionist technology.
Your platform tells you how many calls it answered. It does not tell you how many converted to appointments. It does not tell you how many patients disengaged during the conversation, or why. It does not show you which call types (new patient, emergency, treatment follow-up) are converting at different rates, or flag which times of day or days of the week are producing your worst conversion outcomes.
If your AI dental assistant can produce a call volume report but not a conversion rate report, you are flying blind. Call volume is a vanity metric. Conversion rate is the number that determines whether your practice is growing or slowly bleeding revenue through a leak you cannot see.
Ask your current vendor for a conversion report — specifically, the number of new patient calls received divided by new patient appointments scheduled, for the last 30 days. If they cannot produce it within 24 hours, that tells you everything you need to know about the depth of their analytics capability.
Warning Sign #2: Patients Still Complain About the Phone Experience
If you are still hearing feedback like "I couldn't get anyone on the phone," "the system didn't understand what I needed," or "I just gave up and called somewhere else" — your AI tool is not doing its job.
A well-implemented virtual dental receptionist should reduce friction, not create it. Patients who encounter an AI system that loops them through the same menu options, fails to understand a question about their insurance, or cannot book an appointment because of a scheduling conflict should not be left hanging. They should be smoothly handed off to a human team member, or given a clear path to resolution that preserves the relationship.
The patient experience on the phone is often the first real interaction a prospective patient has with your practice. If that interaction is frustrating — even if the call technically got "answered" — you have not solved the problem. You have just moved it downstream.
According to Oral Health Group, a patient who calls with dental pain and reaches a system that cannot help them does not wait around. They immediately call the next practice on their list — and you have effectively paid for their acquisition with your marketing budget and delivered them to a competitor.
Warning Sign #3: Your Front Desk Team Is Still Overwhelmed
One of the core promises of AI call answering for dental clinics is front desk relief — freeing your team from routine inbound call management so they can focus on in-office patient experience, complex scheduling, and treatment coordination.
If your front desk team is still spending the majority of their day fielding routine phone calls, one of three things is happening: the AI system is not handling the calls it should be handling, the handoff protocol between the AI and your team is poorly configured, or the system is creating more follow-up work than it is preventing.
All three are fixable — but only if you know which one is occurring. That requires data. And the data requires a platform sophisticated enough to track what happens after every call, not just that the call was received.
The dental industry staffing crisis makes this even more urgent. A 2024 DentalPost Salary Report found that over 50% of dental professionals are actively or passively seeking new positions. Turnover costs run $11,000–$14,000 per receptionist. If your AI system is not genuinely reducing the burden on your front desk, you are not protecting your team from burnout — and you are not protecting your practice from the cost of replacing them.
Warning Sign #4: New Patient Volume Has Not Improved
If you implemented an AI call answering system specifically to capture more new patients — after-hours callers, peak-hour overflow, patients who previously hit voicemail — and your new patient numbers are flat three to six months in, something is broken.
The most common culprits:
The system is answering but not converting. The call gets picked up, but the patient disengages during the conversation because the AI cannot handle an insurance question, communicate warmth, or guide the patient toward booking. This is the answering-vs.-understanding gap. The system technically fulfilled its primary function. It just did not fulfill the purpose you bought it for.
The handoff to scheduling is failing. The AI books a tentative appointment, but the data does not sync properly to your practice management system. Your team has to manually process the booking, or worse, the appointment falls through entirely because no one knew it had been made.
After-hours callers are still not converting. Research from TrueLark shows that after-hours calls convert at lower rates even when an AI system picks up — because conversion requires more than answering. It requires the ability to handle objections, explain services, communicate next steps clearly, and leave the patient feeling confident in their decision to book.
DentalBase ROI research found that practices implementing AI call handling recover 60–80% of previously missed opportunities — but only when the system is properly configured, deeply integrated with the PMS, and designed for conversation quality, not just call coverage. Flat new patient numbers after implementation almost always indicate one of these three elements is missing.
Warning Sign #5: You Are Not Getting Coaching Recommendations
The best dental AI assistant tools do not just handle calls — they make your human team progressively better at handling the calls that require a human.
If your current system is not surfacing moments where a team member missed a conversion opportunity — a price objection that was not addressed, an insurance question that was answered with uncertainty, an emergency case that was not triaged with appropriate urgency — you are missing half the value of what AI can deliver in a dental front office context.
Coaching is where the compounding value lives. A team member who receives specific, call-level feedback ("at 2:14 of this call, the patient asked about insurance and paused — here is how a top performer would have responded") improves measurably over time. A team member who receives a general quarterly review based on anecdotal observation does not.
At scale — particularly for emerging DSOs and multi-provider practices — the difference between a team that receives automated, data-driven coaching and one that does not is the difference between consistent conversion rates across all your providers and wide, unexplained variability that you cannot diagnose or fix.
Warning Sign #6: You Cannot Connect Call Performance to Revenue
This is the most sophisticated warning sign, and the one most practices do not realize they should be asking about.
Your AI call tool should be able to tell you not just that a call converted to an appointment — but what that appointment was worth, whether the patient showed up, whether they accepted the treatment plan, and how that individual call contributed to your monthly production.
Without that connection, you cannot answer the question that every marketing and operations decision in your practice ultimately hinges on: which calls are generating revenue, and which are not — and what is the difference between them?
Peerlogic's data shows that for DSOs, 38% of revenue flows through phone conversations — making phone performance not an administrative function but a core revenue driver. A tool that manages that channel without connecting it to production data is not giving you what you need to manage your practice intelligently.
The Deeper Issue: Most Tools Are Answering, Not Analyzing
The fundamental problem with the majority of dental AI receptionist products — including some that are well-marketed and heavily funded — is that they were built around call handling, not conversation intelligence.
Answering a call and understanding a call are not the same thing.
A basic AI call answering service for dental clinics can transcribe a call. A more sophisticated virtual receptionist can route a call. But only a conversation intelligence platform can tell you what that call meant for your revenue cycle — what the patient was actually trying to communicate, where they disengaged, what would have changed the outcome, and how to ensure the next team member who fields a similar call handles it differently.
This is where Peerlogic takes a fundamentally different approach. Rather than focusing solely on the answering layer, Peerlogic analyzes every conversation for patient intent, objection patterns, and conversion likelihood — then surfaces that intelligence for your team in real time and over time.
What to Do If Your Current Solution Is Failing
Step 1: Request a conversion report. Ask your vendor for new patient calls received vs. new patient appointments scheduled over the last 30 days. Not call volume — conversions. If they cannot produce it, you have your answer about the depth of their analytics.
Step 2: Audit the patient experience. Have someone call your practice as a mystery shopper — both during and after business hours. Note where friction occurs, where questions go unanswered, and whether the experience inspires confidence.
Step 3: Check your PMS sync. Pull your appointment log for the last month and compare it against the calls your AI system reports as "booked." Identify any discrepancies. These gaps represent real patients who thought they had an appointment and did not.
Step 4: Ask about coaching capabilities. Ask your current vendor whether the platform flags specific calls for manager review, surfaces coaching moments to team members, or provides any structured performance improvement workflow. If not, you are using a call handling tool — not a revenue optimization tool.
Step 5: Model the revenue gap. Using industry benchmarks: if your practice receives 80 new patient calls per month and converts 42%, you are booking approximately 34 appointments. If a better platform raised that to 55% conversion, you would book 44 appointments — 10 more per month, at $850 per patient in immediate revenue. That is $8,500 per month in recoverable revenue. Over a year, $102,000. That math is the reason the right platform decision matters.
What to Look For Instead
When evaluating a replacement or upgrade, the criteria that actually matter are:
Conversion analytics, not just call logs. Can the platform tell you your new patient call conversion rate by day, by call type, by team member, and by location?
Coaching capability. Does it automatically flag calls where a team member missed a conversion opportunity and deliver specific, actionable feedback?
Deep PMS integration. Does appointment data flow both directions — reading availability and writing confirmed bookings — without manual reconciliation?
Revenue cycle connection. Can you see how call performance connects to production data, treatment acceptance rates, and patient lifetime value?
HIPAA compliance documentation. Can the vendor produce a BAA, consent notification language, and data retention policies on request?
Peerlogic was built for practices that have already tried the basics and are ready for something that actually moves the needle. The practices generating the best results are not the ones with the newest phone technology — they are the ones with the deepest visibility into what is happening in their patient conversations and the most systematic process for improving it.
One practice using Peerlogic in combination with Scheduling Institute's training booked 244 additional appointments, generating over $204,000 in additional annual revenue — not by spending more on marketing, but by converting more of the calls they were already receiving.
Frequently Asked Questions
How do I know if my AI dental receptionist is actually working?The clearest indicator is conversion rate — new patient calls received vs. appointments scheduled. If your platform cannot report this metric, you have no reliable way to measure performance. Other indicators: patient complaint rates, front desk workload, new patient volume trends after implementation.
What is a good call-to-appointment conversion rate for a dental practice?Top-performing practices convert 55–75% of answered new patient calls to appointments. Industry average is closer to 42%. If you are below 42%, your phone process — AI or human — has a significant optimization opportunity.
Can I use Peerlogic alongside my existing AI call tool?Peerlogic's conversation intelligence layer can complement existing call handling infrastructure in many cases. Contact Peerlogic directly to discuss your current setup and what an integration would look like.
How quickly can I see results from switching to a better platform?DentalBase research indicates most practices see positive ROI within 4–8 months, with meaningful performance improvements typically visible within the first 30–60 days of full deployment.
Is the problem my AI tool or my front desk team?Usually both — and the answer is exactly what conversation intelligence is designed to reveal. The right platform will show you precisely where AI call handling is falling short and where human team performance is the limiting factor.
→ Request a practice analysis to see where your current setup is leaving revenue on the table.→ See how Peerlogic's conversation intelligence platform works for dental practices of all sizes.→ Request a demo to see Peerlogic's patient acceptance data in action.
Sources: Peerlogic / Scheduling Institute | Resonateapp.com | TrueLark 8M Conversations | DentalBase ROI Guide | DenteMax | DentalPost 2024 Salary Report via AADOM | Oral Health Group | New Patients Flow | Arini.ai | TrueLark DSO Trends

.svg)
.svg)
.svg)
